

Many factors influence the patient throughput in and out of the Emergency Department. Clarity in layout and simplicity in operations are keys to streamlined flow.
The Emergency Department (ED) has become the ‘Front Door’ to the hospital. Many institutions report that 50 per cent or more of their admissions come through the ED. Yet in many hospitals the flow to and through the ED is fraught with bottlenecks, with confusing and conflicting messages circulating to and within the ED. Hospitals with only one or poorly placed dual entrances experience the chaos of co-mingling of self-arriving patients with those coming in emergency vehicles. Many EDs have poorly conceived first encounter systems. For instance, triage stations that are too small or too few result in patients lining up to be seen, in effect, diluting or even negating the concept of priority screening. Or, queuing can also build up if distinct patient registration stations are adjacent to the waiting room. Poorly designed treatment areas inhibit efficient clinical operations. There are many examples of layouts that require excessive walking to fetch supplies, to get patients to an x-ray room, or to simply manage the patient record. These conditions lead to delays in treatment and increased length of stay within the department, which in turn lead to the build-up of stress in patients and staff alike. Poor and inefficient patient throughput results in costly, error-prone operations and patient dissatisfaction.
There are two ways to come to the ED. Most of us envision going to the ‘Emergency Room (ER)’ as that dramatic, frenetic trip we see depicted in movies and on television in an ambulance with the siren blaring. The by far more common occurrence is to be brought by family, friends or come alone. We distinguish these two arrivals as ambulance and ambulatory or self-arrival
Initially, the ‘ER’ had but one entry. The ambulance arrivals and the ambulatory patients alike came in this way. Of course, as the hospital’s emergency services grew, more and more people began to access the service and this entry became highly congested, chaotic and, quite simply, unsafe. Fundamental change in the layout of the ED began to manifest separate entrances for the two types of traffic. These entrances were generally side-by-side, and indeed, many instances of this arrangement are in use today. Having these in close proximity, however, still creates an opportunity for confusion and uncertainty for the self-arrival patient as to which is the correct place. The optimal layout is to have distinct pathways for the ambulance apart from the ambulatory. This separation should begin at the arrival to the campus and continue to each entry. Ideally, the ambulance entrance should be located so as not to be in sight from those coming to the ambulatory entry. Signage and directions to the Emergency Department should point only to the Ambulatory Entrance—ambulance drivers and emergency medical technicians are familiar with the route and don’t require such directions. This arrangement eliminates the need for the self-arriving patient to make choices regarding which entry may be correct.
The Ambulatory Entrance should be unmistakably obvious and have a system to shelter arriving patients from the elements. Doorways should have hands-free operation and a supply of wheelchairs should be readily accessible. There should be someone from the hospital available at this point to assist the patient into the hospital. This is often done by security personnel.
The advent and utilisation of the electronic health record brings a significant opportunity to streamline and improve patient flow. When a ‘paper’ chart is used, the patient record must remain in close proximity to the unit clerk, who manages the upkeep of the record. Since doctors, nurses and ancillary care-givers must access this same, unique, singular set of documents, there are frequent occasions when the location of the chart is difficult to determine and much time is wasted by care-givers looking for it. The electronic record allows data to be entered anywhere within the unit, especially at the patient bedside. Multiple, simultaneous access permits faster entry and retrieval of data from within the unit and from remote diagnostic services such as the lab.
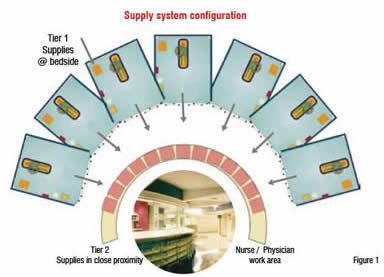
An axiom of the workplace holds that worker efficiency has direct relationship with the placement and availability of supplies. The same holds true in the healthcare environment, especially in the ED, where patient throughput is impacted by the nurses’ ability to get needed supplies at the bedside. It is clear that if much walking is required to fetch supplies from centralised clean supply and utility rooms, more time will elapse in the patient visit. Moreover, evidence now shows that when nurses spend a lot of time walking, this can result in increased stress and concomitantly decreased effectiveness in direct patient care. When supplies are decentralised and evenly distributed throughout the department, walking distances are reduced and access time is improved. A three-tier supply system has proven to be highly successful in supporting improved throughput. The first tier system includes items common to each bedside, alcohol wipes, blood draw tubes etc. The second tier system, which includes items like procedure trays, IV fluids, assorted catheters etc., is essential to this concept. These items must be located within just a few steps from the patient bedside. An often used configuration is to have the second tier supply in carts or cabinets at the perimeter of the nurse and doctor work area that is in the centre of an array of exam rooms or patient care stations. A central storage room, the third tier supply system, is located on the unit out of the area of direct care. This is where infrequently used items and backup supplies for Tier 1 and Tier 2 are kept.
Getting diagnostic information in a timely manner has significant impact upon patient flow through the ED. A high per centage of patients require x-rays. Sending the patient to the Radiology Department has become too onerous in terms of time—transport time, queuing in the department, waiting for a radiologist’s reading and so on. The quest to improve patient throughput has resulted in placing medical imaging within the ED. The volume of patients seen in the department will, of course, determine the number of radiographic devices required, but in high volume EDs, multiple devices can be expected. As in the case of decentralised supplies, the same benefit of improved throughput will accrue from decentralisation of diagnostic tools, especially if digital radiographic devices are used. Since digital medical imaging is filmless, multiple devices need not be clustered for operational efficiency. Placing a DR in proximity to the ‘fast-track’ zone will greatly increase turnaround time for image acquisition and result in quicker diagnoses. A second DR can then be placed conveniently to serve the more acute patient. Placing a CT scanner adjacent to trauma bays saves critical time in dealing with life-threatening situations.
After medical clearance by the emergency medicine physician, the patient and his family / escort is either given discharge instructions and is released to leave the hospital or is admitted to the hospital. If the patient is admitted, several steps must be taken to place the patient in a bed. The timeliness of moving the patient out of the ED and into this bed will greatly affect the overall patient flow in the department. If location and assignment of beds is slowed or beds can’t be found, these admitted patients become ‘boarders’ in the ED. Boarded patients then occupy space that could be used to treat the next incoming patient and in effect reduce the number of beds available to do so. Just a few unexpected ‘boarders’ can choke an organised flow through the ED.
The disposition of inpatient beds is a complex issue, but it is imperative that the hospital be committed to a policy of timely bed availability for those in need.
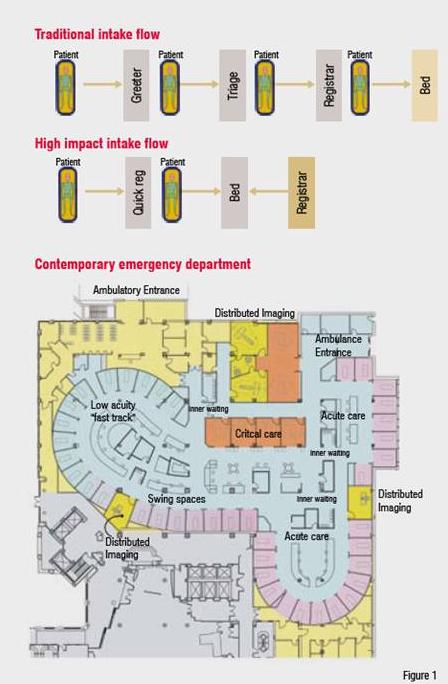
Immediately upon arrival, the ambulatory patient must be acknowledged and given the opportunity to state his problem. This is done by a non-clinical “greeter” who conducts ‘quick reg’ (registration)—a basic set of identifiers to register the patient into the hospital’s record system. This should take but a few minutes. When beds are available, the patient is placed immediately therein. The registration process can be completed at the bedside.
But, what to do when the beds are all full? After the quick reg, the patient is given an initial assessment by a clinician—generally a nurse in a triage station. This triage will determine the severity of the patient’s condition and allow the emergency personnel to establish the priority to provide care. The patient, and in many cases with family members or escorts, is then shown to an ‘inner waiting area’ in the treatment zone. The patients can be watched and reprioritised, thereby getting the right patients into a bed more quickly. The traditional concept of a main waiting room is altered. Since patients and some family members are waiting within the treatment areas, the main waiting room can be much smaller, as it will be serving family and visitors who shouldn’t be or prefer not to be accompanying the patient.
To improve patient flow, a scheme for treating patients with low-risk problems such as sprains and lacerations should be developed. This notion of a ‘fast-track’ should be incorporated within the context of the total treatment area. All beds should be capable of severing any acuity level. The fast track patients can be clustered in one area of the overall department not isolated in a discreet or separate unit. This will permit flexibility in assigning patients to rooms based upon the variation in volumes throughout the day.
Ambulance patients have a different track into the ED. The condition of these patients is generally communicated to the ED by the ambulance personnel—paramedics or emergency medicine technicians. Their arrival is then anticipated and care protocol can be promptly implemented. However, there are occasions when multiple arrivals occur at essentially the same time. When this happens, a triage of these incoming patients becomes necessary. In high-volume EDs, especially trauma centres, planning for an ambulance triage station will afford appropriate space to handle this traffic.










