Covid-19 Pandemic
The challenge of quality patient care in hospital systems

The Covid-19 pandemic has made achievement of patient care in hospital systems an anachronism. Most hospital employees have lost interest and hope that improved excellence in patient care is achievable because of the general belief that top management lacks the skills to identify and constructively adapt to new medical challenges that require rapid response. Furthermore, healthcare workers feel neglected, poorly paid and often ignored when their ideas trickle up to those at the top. It is hellishly frustrating that middle management is even less qualified in the redesign and preparedness in focusing on processes and systems that drive employee motivation and patient care. The paper through the use of a case study suggests a practical approach to the implementation of Total Patient Care (TPC) in healthcare; a Systems Management approach..
The author is of the opinion that TQM is a process which embraces the conscious striving for zero defects in patient care and caring; the management of hospital organisations in co-operation with its workforce to improve processes in order to develop, produce and provide all medical services which satisfy patients’ needs and expectations. Although this represents a meaningful, detailed definition of TPC, Haigh and Morris (1994) contend that most managers find it impossible to work co-operatively with their employees to achieve improved organisational performance. This is because the structural adjustments are usually at odds with processes and patient outcomes as we have seen with lack of hospital capacity and mortality rate for Covid-19 patients. To achieve excellence, I am of the opinion that organisations must first map the business terrain by breaking down the organisation into three key elements: Figure 1.

Explaining the TPC Implementation Approach
The author’s suggestion, therefore, is that quality patient care is fundamentally a structural decision determined at corporate level and must trickle down to all employees in cross-departmentally staffed medical cells. The structure must be focused on dedicated factories for dedicated medical care and resolution. Its success is dependent on middle management having a total buy-in and effectively implementing it with a proper thought out plan; with clearly defined quantifiable goals, roles and responsibilities for individual units, and having in place organisational norms that emphasise listening, supporting, coaching and rewarding staff appropriately. It should be noted, however, that at the initial stage of implementation, the success of TPC is not dependent on senior management commitment, but on a proper and effective implementation strategy championed by middle management, endorsed and made to work by a happy workforce, which would then have a domino-effect across the whole organisation.
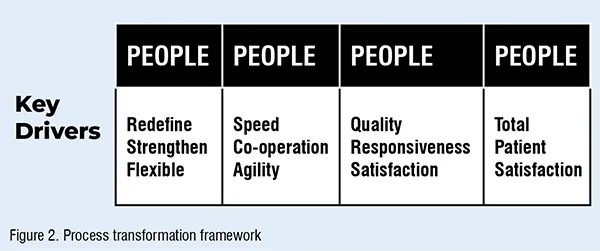
TPC is akin to playing basketball; it is simple, but we choose to make it complex by being overly technical. TPC is essentially a way of organising and involving the whole organisation; every department, every activity, every single person at every level focusing on the organisations’ core competencies in order to deliver continuous value to the patient. To that end, the authors suggest the use of a theoretical operations-based transformation framework at the onset of TQM as a guide for the identification of areas for improvement (Figure 2).
TPC is About the will and the way of the People
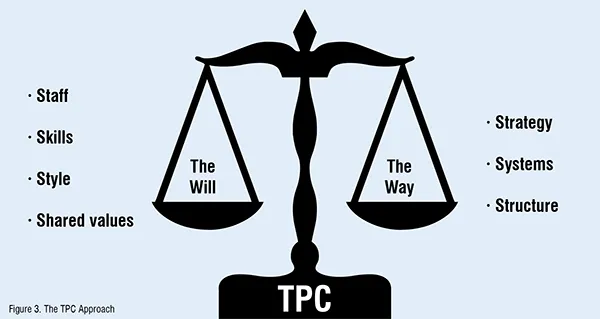
The sustainable transformation of an organisation to a TQM culture, in the authors’ opinion, requires a balance between organisational strategy, systems and structure (the way) with the fundamental commitment of staff, their skills, managerial style and values (the will): Figure 3.
Without the development of the will, the ongoing success of the TPC programme would require a large amount of attention, effort, and energy to work against the fundamental status quo in an organisation, which dictates that ‘things should be done the way they have always been done’. The will can only be generated if TPC is accompanied by a plan to ensure that the behaviours encouraged are aligned with those required by the culture. Furthermore, as identified by the author the ‘WILL’ for ‘TPC’ must be fully developed by ensuring professional competencies are at the highest level and paying employees above market rate. The way is focused on servant and authentic leadership. Therefore for TPC to succeed, a ‘total’ re-orientation of employee beliefs and values is required. This is consistent with the views of Thomas Watson, Sr., the founder of IBM, who noted, “Any great corporation, one that has lasted over the years, will find it owes its resilience not to its form of organisation or administration, but to the power of values and beliefs and the appeal these values and beliefs have on its people (Arikian, 1991).
E-Hospital Case study Background
E-Healthcare came into existence on 1 August 2018. In total, E-Healthcare is responsible for an expenditure of US$560 million on health services, for its community. The main work of the E-Healthcare is to:
- assess the health needs of the local population and identify health problems in the area
- draw up a strategy for meeting those needs and dealing with particular problems
- provide medical services to meet patient needs in the most effective and cost efficient way
- monitor the provision of services to ensure that standards and targets are being met.
E-Healthcare employs a staff of about 2,200 across 5 hospitals, including part-time and seconded staff. The managerial structure of the organisation comprises of the chairman and five non-executive members of two statutory authorities and a jointly appointed chief executive. Their role is to oversee matters of policy and strategy, to monitor performance and ensure that the organisation operates to the highest standards of probity and accountability.
- Hospital 1; provides medical, surgical, maternity, child health and pathology services
- Hospital 2; provides community care, and also cares for people with mental illness or severe learning disability
- Hospital 3; is responsible for treatment and care for people with cancer
- Hospital 4; provides a wide range of hospital based medical and surgical services,
- Hospital 5; also provides medical and surgical care.
Reasons to Switch to TPC
The organisation had to cope with the new changes that have been taking place to demonstrate an organisation wide approach to improving the quality of patient care through the development of quality improvement strategies which should be made explicit in business plans”.
Secondly, due to increased competition, the chief executive felt that the adoption of TPC would bring about a new cultural perspective that enhanced the need to provide medical services that meet the needs of the local community in terms of quality, speed, access, effectiveness, efficiency, comprehensiveness, safety, and appropriateness.
Furthermore, there were underlying barriers to be surmounted by recourse to the implementation of TPC within the organisation:
- poor communication between staff of the organisation and management
- lack of trust amongst administrators and clinical staff.
- medical interventions not clinically effective, i.e. 70 per cent of hospital procedures not clinically proven.
- failure to address and meet local needs: demographic shifts. In addition, patients are chosen on the basis of colour and not equity as is presently the case with Covid-19 vaccination.
- lack of customer awareness: at this stage the word ‘customer’ was alien to the organisation’s staff; hence, improper patient assessment.
- financial management top priority; lack of patient value.
All of these factors had driven the management of E-healthcare to go down the TPC route. The organisation, therefore, through the adoption of total patient care, aims to ensure the provision of services which;
Structure
- are effectively managed withappropriately trained staff
- have clearly defined quality assurance and service review policies and guidelines
- are based on a systematic assessment of local needs.
Process
- promote good health and healthy living
- support people with continuing disabilities and ensure relief is provided for their carer
- are accessible and timely for all sections of the population in the county
- achieve equity between different patient social and geographical groups
- ensure communication with individual consumers and the wider community about all aspects of the care provided and the services available.
- encourage and take into account the high aspirations of staff in all disciplines.
Outcome
- make the most efficient and effective use of resources
- are sufficiently documented to facilitate continuity of care and peer evaluation
- achieve effective outcomes in the prevention and treatment of disease and rehabilitation
- improve the patients’ subsequent quality of life
- ensure the consumer receives an acceptable standard of care at all times.
In the words of the patient care manager, the TPC programme was based on three major dimensions: Figure 4.
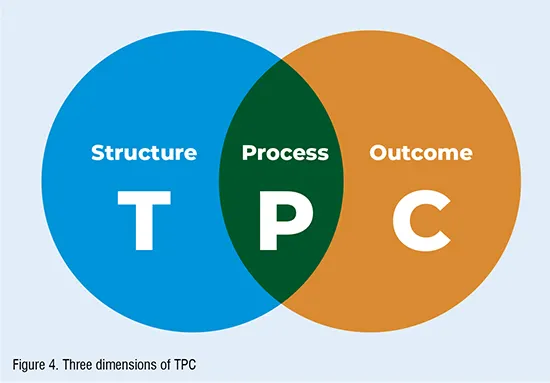
Quality, the manager suggests, “cannot be considered in isolation, as it is influenced by a range of factors: professional standards and aspirations, technical competence and skills, attitudes and social behaviour, consumer expectations and the resources available. Hence, all persons involved in the delivery of care, and the provision of support services, are key to the achievement of a high quality service”.
TPC Implementation Stages
Stage 1:
The organisation had to first identify and adopt a clear vision based on what their main business and purpose is. According to the Patient Care Manager, the main purpose of the organisation is to “purchase the ‘best’ quality service for its patients”. The adoption of a vision based on the purchase of quality services provided clarity of purpose for all staff to work towards. In addition, a decision was taken by senior management not to introduce TPC as top management’s top-down rule, but as a home-grown approach where employees were allowed to voice their scepticism and make suggestions. Thus, employee involvement was seen as the first initial requirement of the TPC process.
Stage 2:
Involved the setting up of focus groups to identify gaps in service provision from the patient perspective. The focus group carried out a patient satisfaction survey across the county, which established a number of gaps:
- fear of retribution
- long waiting times at hospital outpatients
- poor catering services
- clinical outcomes – performance judged by peers rather than by patients.
On the basis of the patient survey, the organisation set out nine strategic priorities to deal with and close the gaps that were identified in the provision of services. The strategic intents included:
- establishing primary care and cancer treatment as the principal focus
- reshaping hospital provision to meetthe changing health service needs of the population
- implementing ‘the health of the nation’ through the achievement of health goals and targets to improve the health status of the population
- ensuring the successful implementation of community care act through effective collaboration and joint action between social services and health services and other organisations
- ensuring that inpatient and outpatient waiting times meet and exceed agreed standards.
- ensuring continued value for money through efficient and effective use of resources to achieve health gains
- empowering consumers through the implementation and further development of the patients charter
- establishing a comprehensive research and development programme
- creating an effective organisation able to deliver changes in primary, community and hospital care services.
‘Quality Care is meeting patients’ needs’.
To cascade this definition across the organisation required a new organisational culture emphasising:
- a customer orientated focus
- top management (including clinicians) commitment to quality
- the involvement of all staff in quality development and delivery
- incremental/continuous quality improvements each and every year.
This new culture was to be sustained through an adherence to three core values: monitoring performance against agreed quality requirements between the organisation and its service providers; strengthening focus and developing patient empowerment developing quality medical cells and empowering staff.
The new system, according to the contracts/purchasing manager, enabled the organisation to deal with the initial barriers prior to TPC. To further ensure the internalisation of the three core values, the organisation made it mandatory for all its service providers to identify their corporate approach to quality and the responsibilities within their organisations for quality improvement, firmly linking these to their strategic objectives and translating them into key tasks and work programmes for each year. In addition, E-Healthcare asked a committee of employees to monitor progress during the year and evaluate clinical outcomes, which in turn informs the following year’s plans and programmes. To ensure compliance, the organisation introduced a uniform quality approach to be adopted (Figure 5).

Using the above diagram as an illustration, what the case study seems to suggest is that for TPC to succeed, hospitals must work in partnership with its suppliers of service (inputs), involve patients and employees in the improvement and redesign of processes, in order to meet their expectations, which would result in the provision of a quality service (output). This requires the realignment of the entire organisational system to the principles of TPC, thereby creating a quality environment in which those with the primary responsibility for the treatment and caring of patients will work in concert. Any TPC implementation process that falls short of integrating and involving the ‘whole’ system would result in the partial implementation of TPC. A system is not the sum total of its parts, but the interaction of the whole.

