The Next Frontier in Cardiothoracic Transplant Surgery

Dr. Ahmed Mohamed Kamel Mohy Eldin Omar Rslan,Resident, Department of Cardiothoracic Surgery, Qena University Hospital, South Valley University
Dr. Ahmed Mohamed Kamel Mohy Eldin Omar Rslan is a Resident in Cardiothoracic Surgery at Qena University Hospital, South Valley University, Egypt. His professional interests include cardiac surgery innovation, thoracic trauma management, and clinical research. He is committed to advancing surgical education and improving patient outcomes in cardiothoracic practice.
Abstract
Cardiothoracic transplant surgery is changing rapidly with advances in technology, donor management, and surgical care. This interview explains new protocols, organ preservation, and team-based approaches that improve survival. It also highlights regional challenges in Asia and future innovations like ex-vivo perfusion, xenotransplantation, and regenerative medicine, offering a complete view of this complex field.
1. How has the field of cardiothoracic transplant surgery evolved over the last decade in terms of clinical protocols, surgical innovations, and technology? In what ways have these advancements - particularly in perioperative care - contributed to improved patient survival and outcomes?
In the last decade, cardiothoracic transplant surgery has improved a lot. Fast-track anaesthesia and better monitoring made operations safer and recovery faster [1]. New surgical techniques, such as minimally invasive incisions and improved anastomosis, reduced operative time and improved graft function. Donor management and organ preservation, especially ex-vivo perfusion, increased the number of usable organs [3]. These advances improved survival, lowered complication rates, and gave patients a better quality of life. Today, heart and lung transplantation is safer and more predictable than before.
2. What are the current primary indications for heart and lung transplantation, and how has the process of patient selection improved with advances in diagnostics and risk stratification?
Heart transplantation is usually for patients with end-stage heart failure, severe cardiomyopathies, or complex congenital heart disease [1]. Lung transplantation is used for conditions like COPD, pulmonary fibrosis, cystic fibrosis, or pulmonary hypertension [2]. Modern tools, including imaging and biomarker testing, make patient selection more accurate. Doctors now look at comorbidities, physical ability, and psychological readiness before listing a patient. This helps to choose the right time for surgery, lower the risks, and improve long-term survival and recovery after transplantation.
3. Organ scarcity remains a critical challenge. What innovative donor management or organ preservation strategies are being used to expand the donor pool, especially in Asia?
Organ shortage is still a big problem in Asia. Cultural and religious issues reduce donation rates, and not all countries have strong systems for organ sharing. New donor protocols, such as hormonal therapy and haemodynamic optimisation, allow use of more donors. Ex-vivo perfusion makes it possible to use marginal or distant organs [3]. Public education and new laws are slowly improving donation rates. Regional networks for organ sharing could also help. These steps are very important to meet the growing need for heart and lung transplants in Asia [2].
4. How have ex vivo organ perfusion technologies transformed your approach to cardiothoracic transplantation - particularly in terms of organ viability, transportation logistics, and postoperative outcomes?
Ex-vivo perfusion has changed organ transplantation. It keeps hearts and lungs alive outside the body, which means longer preservation and better assessment of organs before surgery [3]. This reduces the number of discarded organs and allows the use of marginal donors. Patients benefit through lower risk of primary graft dysfunction and improved outcomes. It also gives doctors a chance to repair or condition organs before use. Ex-vivo perfusion is now one of the most important innovations in modern transplant surgery [4].
5. What role does pre-transplant optimisation - such as nutritional support, respiratory rehab, and cardiac conditioning - play in enhancing transplant success? Are more structured protocols emerging in this space?
Preparing patients before transplant is key for better results. Nutrition support helps patients who are weak or underweight. Pulmonary rehabilitation improves breathing, and physiotherapy strengthens muscles. Psychological support also prepares patients for the stress of surgery. These steps reduce ICU time and complications after transplant [1]. Today, most centres use structured multidisciplinary programmes, including dietitians, physiotherapists, and psychologists. Personalised plans are made for each patient depending on their health condition. This makes recovery faster and survival higher in the long term.
6. What are some of the most technically challenging aspects of heart and lung transplantation surgery? How do you approach decision-making when balancing surgical risks with the patient’s clinical urgency?
Heart and lung transplantation is technically difficult. Problems like size mismatch between donor and recipient, adhesions from previous surgeries, and fragile tissues make surgery complex [2]. Intraoperative instability and bleeding can occur. Surgeons must balance urgency with risk, often with team consensus. The quality of the donor organ and recipient's health guide decisions. In high-risk cases, backup plans like ECMO or staged procedures are prepared. Success depends on precision, planning, and flexibility in surgery [4].
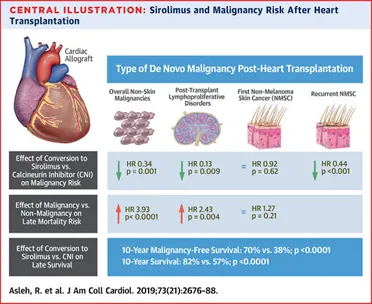
7. How is the field moving toward more individualised immunosuppressive regimens to reduce long-term complications such as chronic rejection, infections, and malignancy?
Immunosuppression today is more personalised than before. Doctors use genetic and metabolic information to choose the best drugs and doses for each patient [1]. Lower doses of calcineurin inhibitors reduce kidney problems, while adding mTOR inhibitors or cell-cycle agents gives balance. Regular monitoring of immune function reduces infection and rejection risks. Preventive strategies against cancer and infections are also part of long-term care. This personalised approach improves graft survival and helps patients live longer with fewer complications [5].
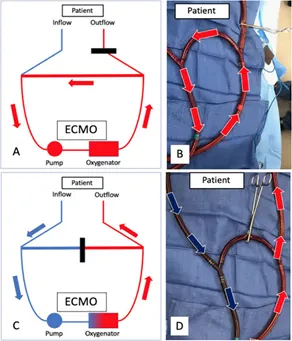
8. With Extracorporeal Membrane Oxygenation (ECMO) increasingly used as a bridge to transplant, what criteria or protocols guide its application in your practice? How do you assess its risks and benefits?
ECMO is often used as a bridge to transplant in patients with severe heart or lung failure [2]. It supports patients until a donor organ becomes available. Selection is important—patients must not have severe multi-organ failure. The goal is to keep ECMO duration short to avoid complications like bleeding and infection. Daily team assessments guide decisions, adjusting support as needed. If used carefully, ECMO stabilises patients, improves their condition before surgery, and leads to better results after transplant without raising major risks.
9. Re-transplantation presents complex clinical and ethical questions. What are the main factors you consider when determining whether a re-transplant is appropriate?
Re-transplantation is rare and complex. It is usually done when the first graft fails due to rejection or primary dysfunction [5]. Doctors must carefully consider organ scarcity and fairness in allocation. Sensitisation, previous surgeries, and patient condition affect eligibility. The decision is made by a multidisciplinary team to ensure fairness and the best use of available organs. Only patients with a high chance of good recovery are chosen. This protects both patients and the transplant system.
10. What are the specific challenges associated with pediatric heart and lung transplantation? How do considerations such as organ size, growth potential, and long-term follow-up influence treatment planning?
Children needing heart or lung transplants face unique problems. Donor organs are fewer, and size matching is difficult [2]. Surgeons must adjust techniques for small anatomy and future growth. Immunosuppression is tricky, as strong drugs can affect growth and development. Long-term follow-up is essential, including physical, social, and emotional care. Paediatric transplant teams include cardiologists, pulmonologists, dietitians, and psychologists. They make sure children adapt well, grow properly, and move smoothly into adult care. Holistic and team-based care is the key to success.
![]()
11. How critical is the role of a multidisciplinary team - including cardiologists, pulmonologists, intensivists, infectious disease experts, and psychologists - in delivering successful transplant outcomes?
Successful transplantation needs many specialists working together. Cardiologists and pulmonologists prepare patients, intensivists manage perioperative care, and infectious disease doctors prevent infection [1]. Psychologists support patients mentally, while physiotherapists help in recovery. Regular meetings improve teamwork and patient safety. This cooperation makes outcomes better, and patients feel more supported. The strength of a transplant programme depends on the quality of its team and the integration of all disciplines into one plan of care.
12. What are the region-specific challenges faced by Asian countries in advancing cardiothoracic transplant programs - such as infrastructure gaps, funding limitations, or cultural barriers to organ donation?
In Asia, many challenges still exist. Donation rates are low due to cultural issues, and some countries lack infrastructure and funding [2]. Advanced technology like ex-vivo perfusion is not always available. Trained transplant teams are limited in some areas. Solutions include stronger public education, national sharing systems, and sustainable funding models. Policymakers must also invest in training programmes and better facilities. With these changes, more patients in Asia will have access to safe and effective transplant surgery.
13. How close are we to the clinical reality of xenotransplantation or lab-grown organs for heart and lung transplants? What key scientific or ethical barriers must still be addressed?
Xenotransplantation and artificial organs are possible future solutions to organ shortage. Animal-to-human transplantation still has risks like rejection and infection [3]. Stem cell research and gene editing are bringing lab-grown organs closer to reality. Scientists are testing decellularisation and recellularisation techniques. Clinical use is not yet common, and strict regulation will be needed [4]. Large trials and ethical debates must continue before routine use. These innovations may become a major solution in the next decade.
14. What policy changes or healthcare reforms do you believe are necessary to improve equitable access to cardiothoracic transplant services, especially in low- and middle-income settings?
Improving access to transplantation in low- and middle-income countries requires strong policy action. National registries and clear referral systems are needed [2]. Publicly funded transplant programmes reduce financial barriers. Living donor programmes, when safe, can help. Regional sharing improves efficiency. Education campaigns increase donor registration. Fair allocation rules must be applied to avoid inequality. With these policies, more patients will benefit from transplant surgery, no matter their income or location.
15. Looking ahead, what do you see as the most promising trends or innovations that will shape the future of heart and lung transplantation over the next 5 to 10 years?
The future of transplantation looks promising. Ex-vivo perfusion will expand further, making more organs usable [3]. Regenerative medicine and stem cell therapies may help repair organs before or after transplant. Artificial and bioengineered organs may enter clinical practice in the next decade. Robotics and minimally invasive techniques will make surgery safer. Telemedicine will allow long-term follow-up, especially in remote areas [4]. With global collaboration and better policies, cardiothoracic transplantation will become safer, more accessible, and more effective than ever before.

References
- Mehra MR, Canter CE, Hannan MM, Semigran MJ, Uber PA, Baran DA, et al. The 2016 International Society for Heart Lung Transplantation listing criteria for heart transplantation: A 10-year update. J Heart Lung Transplant. 2016;35(1):1–23. doi:10.1016/j.healun.2015.10.023. PMID: 26776864.
- Chambers DC, Cherikh WS, Harhay MO, Hayes D Jr, Hsich E, Khush KK, et al. The International Thoracic Organ Transplant Registry of the ISHLT: Thirty-fifth adult lung and heart–lung transplant report—2018. J Heart Lung Transplant. 2018;37(10):1169–1183. doi:10.1016/j.healun.2018.08.001. PMID: 30293613.
- Ardehali A, Esmailian F, Deng M, Soltesz E, Hsich E, Naka Y, et al. Ex-vivo perfusion of donor hearts for human heart transplantation (PROCEED II): a prospective, open-label, multicentre, randomised non-inferiority trial. Lancet. 2015;385(9987):2577–2584. doi:10.1016/S0140-6736(15)60261-6. PMID: 25888086.
- Messer S, Cernic S, Page A, Berman M, Kaul P, Colah S, et al. A 5-year single-center early experience of heart transplantation from donation after circulatory-determined death donors. J Heart Lung Transplant. 2020;39(12):1463–1475. doi:10.1016/j.healun.2020.07.002. PMID: 32773054.
- Haddad F, Khush K, Valantine H, Kobashigawa JA. Management of the sensitized heart transplant candidate: a survey of current practices in the United States. J Heart Lung Transplant. 2010;29(12):1335–1341. doi:10.1016/j.healun.2010.07.013. PMID: 20869720.

