Advanced Invasive Hemodynamics: Pressure-volume Maneuvers to Obtain Load-Independent Indices
Understanding Hemodynamics through Pressure-Volume Analysis

Haemodynamics has advanced significantly since 1628, with the conductance catheter (1984) enabling detailed pressure-volume measurements crucial for research and clinical practise. Cardiac catheterisation and PV relationships aid in decision-making, while load-independent manoeuvres further assess heart function, enhance detection and assessment of heart failure.

Introduction of current state to haemodynamic research
Haemodynamics, the study of the biophysical principles and laws governing blood flow dynamics, boasts a rich history spanning several centuries. Over 350 years after Harvey’s groundbreaking theory of blood circulation in 1628, Baan and colleagues introduced the first conductance catheter in 1984 (Baan J, 1984). This innovation enabled the simultaneous and continuous acquisition of pressure-volume (PV) measurements in mammals, revolutionising haemodynamic evaluations in preclinical and clinical settings. Today, PV relationships are widely utilised in preclinical (pharmacologic drug R&D, safety, genetic, or mechanical circulatory support) and clinical cardiac catheterisation-labs globally to accurately assess cardiovascular function following various interventions. Despite their profound insights into cardiac function, the routine use of PV catheters in labs remains challenging, requiring a solid theoretical foundation and careful interpretation.
One of the main advantages of using the invasive cardiac catheterisation and the PV relationship, is to capture heart’s blood-volume parameters under full blood load, like in case of other imaging techniques e.g., echocardiography, CT, or MRI. In addition, PV technique provides concurrent pressure data that are synchronised to volume in real time. Moreover, when the blood load is quickly reduced (few techniques available to clinician), mostly in cases of incoming blood load-known as a preload, PV catheter helps to distinguish how the heart muscle and surrounding structures respond to this transient haemodynamic stress. This technique provides further insights into cardiac contractile mechanisms, uncovering possible dysfunction, otherwise unable to be acquired by abovementioned imaging techniques.
Load-independent contractility and limitation of ejection fraction
In clinical terms, cardiac contractility (inotropy) is divided into two main concepts: load-dependant and dose-independent contractility. The Frank-Starling (F-S) law describes how haemodynamic load (preload EDV, afterload MAP or ESP, and heart rate) influences muscle activity. Changes in inotropy adjust the F-S relationship between stroke volume (SV) and left ventricular end-diastolic pressure (LVEDP), shifting the curve up or down. Clinical assessments focus more on blood load rather than intrinsic inotropic properties. To delve deeper into the clinical concept, load-dependant data are recorded as static evidence of contractility/inotropy without further stressing haemodynamic conditions. Within the F-S relationship, changes in inotropy correspond to changes in ejection fraction (EF), a load-dependant parameter. Evidence such as variations in EF, LV dp/dt max, or combinations with maximal aortic flow acceleration (dQ/dtmax) or global longitudinal strain (GLS) from echocardiography provides insights into static load-dependant contractility (Monge Garcia 2018) (Lang 2015). However, this static approach has its considerable limitations. For instance, EF is highly dependant on the assumption of a fixed relationship between ventricular dimensions and volume, which can vary significantly in heart failure situations as there is now a mismatch of dimensions and volume due to cardiac remodelling (Nagueh 2021). Additionally, EF might decrease while contractility increases due to changes in afterload, represented by effective arterial elastance (Ea) (Morimont P 2018). The Ea is a measure used to characterise the arterial load on the heart. It is defined as the ratio of left ventricular end-systolic pressure (LV ESP) to SV. The Ea combines both the steady (resistive) and pulsatile (elastic) components of the arterial load, providing a concise way to assess how the heart and arteries interact (Segers P, 2001). In summary, using EF as the primary clinical index for load-dependant inotropy is limited by the heart chamber’s geometry and the state of the effective arterial elastance (Ea).
Basic load-independent parameters measured in Cath-Lab improving detection of HF
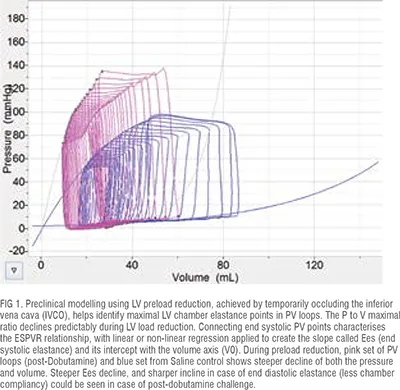
The application of cardiac catheterisation and the use of PV relationships provide a comprehensive view of cardiac mechanics, aiding clinicians in making more informed and effective decisions for patient care. Utilising load-independent manoeuvres further enhances detection capabilities in cases of HF and improves decision-making. It is beyond the scope of this article to list all relevant load-independent parameters that are abnormal in HF, however interested readers could benefit from exploring the listed references further. In HF, changes in the End-Systolic Pressure-Volume Relationship (ESPVR) can indicate impaired systolic heart contractility even when EF appears normal. The ESPVR represents the maximal pressure the LV can generate at any given volume at the end of the systole. When the relationship is established slope of the ESPVR, called the end-systolic elastance (Ees), indicates the systolic contractile strength of the heart muscle (FIG 1). In addition, the intercept (IC), on the volume axis also indicates how the heart muscle behaves during transient load changes (Blaudszun G 2011, Kerkhof PLM 2018). Both must be assessed for a complete understanding of the inotropic changes. Additionally, the position of the initial PV loops before the transient preload reduction occurs needs to be precisely defined on the volume axis, sometimes called the working point (Kerkhof PLM, 2018). Similarly, focusing on the rate of rise of left ventricular pressure (LVP), LV end-systolic pressure (ESP), and pulse wave velocity, a load-independent manoeuvre adjusted afterload (LV ESP) at each cardiac cycle, allows assessment of LV ESP and aortic valve timing. Plotting decaying LV ESP against aortic valve timing reveals a highly linear correlation of both isotonic and isometric contractility improving complexities in the positioning of the PV catheter in the Cath-Lab (Konecny 2022, 2023).
End-diastolic pressure (EDPVR) describes the relationship between the pressure and volume in the left ventricle at the end of diastole (the phase of the heartbeat when the heart muscle relaxes and allows the chambers to fill with blood). This relationship is used to assess the diastolic properties of the heart, particularly its compliance (the ability to stretch and fill). The slope of the EDPVR curve is the reciprocal of ventricular compliance. Fitting the data could be performed to a linear, exponential, logarithmic, or harmonic oscillator models. The most common is an exponential model: P = α(eβV − 1) + P0, where α is the stiffness and scaling coefficient, β is the chamber stiffness coefficient, and P0 offsets pressure at a volume of 0 (Cingolani OH, 2011). In diastolic dysfunction (DD), particularly heart failure with preserved ejection fraction (HFpEF) the heart’s ability to relax and fill with blood during diastole is impaired, even though the ejection fraction remains normal. These changes lead to elevated filling pressures and reduced ventricular compliance, making it harder for the heart to fill properly during diastole. This can cause symptoms like shortness of breath, fatigue, and fluid retention. DD can result from various structural and functional changes in the myocardium, such as altered calcium handling within cardiac cells and increased stiffness of the ventricular walls due to fibrosis or hypertrophy. Interestingly, LV hypertrophy is absent in many HFpEF patients, hence further exploring repetitive pressure overload (RPO) models could offer insight into how diastolic dysfunction and HFpEF may develop in the absence of comorbidities, sustained hypertension, or LV hypertrophy (Weil BR, 2019).
The advantages of the PV exams in clinical settings significantly enhance decision-making by providing detailed and direct measurements of cardiac function, enhancing diagnostic accuracy. In the case of combination of volume and pressure data, it helps in diagnosing complex cardiac conditions e.g. HFpEF or HFrEF, which might not be evident through other methods, leading to more accurate and timely diagnoses. Furthermore, the detailed insights from PV measurements enable clinicians to tailor interventions more effectively. For instance, they can better determine the appropriate treatments for HF or other cardiac conditions based on how the heart responds to different manoeuvring of blood load. Lastly, PV measurements can be used to monitor the effectiveness of in-patient treatments over time (while the catheter is inserted, i.e., continual detection of changes), ensuring that interventions are having the desired effect on cardiac function.
References:
Baan J, van daer Velde ET, dae Bruin HG, Smeenk GJ, Koops J, van Dijk AD, Temmerman D, Senden J, Buis B. Continuous measurement of left ventricular volume in animals and humans by conductance catheter. Circulation. 1984 Nov;70(5):812-23. doi: 10.1161/01.cir.70.5.812. PMID: 6386218.
Monge Garcia MI, Jian Z, Settels JJ, Hunley C, Cecconi M, Hatib F, Pinsky MR. Performance comparison of ventricular and arterial dP/dtmax for assessing left ventricular systolic function during different experimental loading and contractile conditions. Crit Care. 2018 Nov 29;22(1):325. doi: 10.1186/s13054-018-2260-1. PMID: 30486866; PMCID: PMC6262953.
Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, Flachskampf FA, Foster E, Goldstein SA, Kuznetsova T, Lancellotti P, Muraru D, Picard MH, Rietzschel ER, Rudski L, Spencer KT, Tsang W, Voigt JU. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015 Jan;28(1):1-39.e14. doi: 10.1016/j.echo.2014.10.003. PMID: 25559473.
Morimont P, Lambermont B, Guiot J, Tchana Sato V, Clotuche C, Goffoy J, Defraigne JO. Ejection Fraction May Not Reflect Contractility: Example in Veno-Arterial Extracorporeal Membrane Oxygenation for Heart Failure. ASAIO J. 2018 Jul/Aug;64(4):e68-e71. doi: 10.1097/MAT.0000000000000661. PMID: 28953198.
Nagueh SF. Heart failure with preserved ejection fraction: insights into diagnosis and pathophysiology. Cardiovasc Res. 2021 Mar 21;117(4):999-1014. doi: 10.1093/cvr/cvaa228. PMID: 32717061.
Segers P, Stergiopulos N, Westerhof N. Relation of effective arterial elastance to arterial system properties. Am J Physiol Heart Circ Physiol. 2002 Mar;282(3):H1041-6. doi: 10.1152/ajpheart.00764.2001. PMID: 11834502.
Blaudszun G, Morel DR. Relevance of the volume-axis intercept, V0, compared with the slope of end-systolic pressure-volume relationship in response to large variations in inotropy and afterload in rats. Exp Physiol. 2011 Nov;96(11):1179-95. doi: 10.1113/expphysiol.2011.059881. Epub 2011 Sep 2. PMID: 21890525.
Kerkhof PLM, Kuznetsova T, Ali R, Handly N. Left ventricular volume analysis as a basic tool to describe cardiac function. Adv Physiol Educ. 2018 Mar 1;42(1):130-139. doi: 10.1152/advan.00140.2017. PMID: 29446315.
Konecny, Filip. (2022). The Left Ventricular End-Systolic Pressure Correlation with Aortic Valve Timing; a Novel Inotropic Index Description Using a Dual Pressure Catheter. 10.56391/JCCM.2022.1012.
Konecny, F. (2023). Systolic Indices of Cardiac Contractility: Modelling and Analysis using Pressure-Volume Loop. European Journal of Medical and Health Sciences, 5(4), 5–12. https://doi.org/10.24018/ejmed.2023.5.4.1731.
Cingolani OH, Kass DA. Pressure-volume relation analysis of mouse ventricular function. Am J Physiol Heart Circ Physiol. 2011 Dec;301(6):H2198-206. doi: 10.1152/ajpheart.00781.2011. Epub 2011 Sep 16. PMID: 21926344.
Weil BR, Techiryan G, Suzuki G, Konecny F, Canty JM Jr. Adaptive Reductions in Left Ventricular Diastolic Compliance Protect the Heart From Stretch-Induced Stunning. JACC Basic Transl Sci. 2019 Aug 26;4(4):527-541. doi: 10.1016/j.jacbts.2019.04.002. PMID: 31468008; PMCID: PMC6712414.

