Cardiac Surgery
New techniques

The focus of new techniques has been on making cardiac surgery safe, minimally invasive and cost-effective.
Cardiac surgery has witnessed major changes and rapid progress in the last 50 years, since the time of the development of cardiopulmonarybypass (CPB) for clinical use in 1953.Constantly the focus of the improvement in the techniques and technologies has been on making cardiac surgery safe, minimallyinvasive and cost-effective. Major advances have occurred in the fields of off-pump surgery, video assisted surgery, surgical treatment for heart failure, robotic surgery and artificial hearts and prostheses.
Off-pump coronary artery bypass graft surgery (opcab)
In off-pump coronary artery bypass graft,as the name itself indicates, surgery isdone without putting the patient on aheart-lung machine. For nearly 25 years,the standard technique of conventional CABG was to perform it on cardiopulmonarybypass (CPB), i.e. the patient is puton a heart-lung machine.

Cardiopulmonary bypass is an unphysiological state involving alterations in the flow properties of the blood, alteration in thermal regulation, protein denaturation, and exposure of blood to unnatural, non-endothelial surfaces triggering various enzyme cascades such as complement, kinins, coagulation systems and fibrinolytic systems.
There is a great disturbance of the homeostasis leading to various organ dysfunctions, thus accounting for the postoperative morbidity. Also the cost of the operation is high especially in the developing countries because of the cost of the import of various materials required for the conventional CABG on CPB. Hence, in a constant endeavor to make surgery safer for the patients and the attempts to do away with CPB, innovative surgeons with the help and support of the enterprising industries strived together to deal with the dual concerns of risks and cost of conventional CABG. This culminated in the development of Off-Pump CABG (OPCAB).
Off-Pump CABG is minimally invasive as compared to surgery on the heart lung machine. This method eliminates the use of CPB thus avoiding an unphysiological state and permits surgery on multiple arteries within the heart by mechanically stabilising it. The potential benefits include shorter hospital stay, less bleeding, less chance of infection, less risk of irregular heart beats (arrhythmia), less trauma, shorter recovery time, and greater cost-effectiveness. This procedure was initially created to avoid brain injuries attributed to the pump.
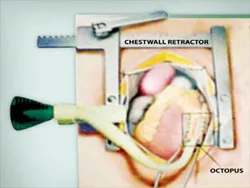
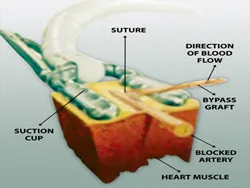
Off-pump CABG is performed with the help of various mechanical stabilisers. They immobilize a small area around the coronary artery for the surgeon to operate while the heart continues to function. The various commercial stabilisers that are available are the Medtronic Octopus device, Guidant suction device, etc.
Off-Pump CABG is further undergoing various modifications of techniques as a result of which many different terminologies and abbreviations are in use. However, the two main principles of OPCAB, minimally invasive and mechanical stabilisation of the heart, remain unchanged.
Minimally invasive coronary artery bypass graft surgery (MICAS)
This refers to all techniques of CABG wherein there is no use of CPB. It also includes operations involving lesser incisions than a standard full median sternotomy.
Minimally invasive direct coronary artery bypass graft surgery (MIDCAB)
MIDCAB or ‘limited access coronary artery bypass’ is usually limited to patients with lesions in one or two coronary arteries, mainly the Left Anterior Descending Artery (LAD) and the Right Coronary Artery (RCA). In contrast with conventional CABG, this procedure is done through a smaller incision on the sides of the patients chest in the fourth left intercostal space and entering the pericardium through the bed of the excised cartilage. This approach avoids making long incisions, splitting of the sternum (breast bone) and subsequently the development of instability of the sternum and infection of the bone and cartilages and also the development of ugly scars (keloid), which is more prone in this location and in dark skinned people.
Lower end sternal split coronary artery bypass graft surgery (LESS)
In this procedure the bypass is done by cutting only half of the breast bone. This is done when there is blockage in one or two coronary arteries. The advantages include fast recovery of patient and quick return to work within 10-14 days.
Thoracotomy Off-pump coronary artery bypass surgery (TOPCAB)
In this procedure a left Antero-Lateral thoracotomy approach is employed. Asian Heart Institute has been a pioneer in LESS, TOPCAB, and OPCAB procedures, which are being done over the last three years with excellent results. Also, Asian Heart Institute is one of the few centers in the world where more than ninety-nine percent of the CABGs are done on beating heart (OPCAB).
Video-assisted port-access mitral valve surgery
In this technique, the breast bone is not opened. The patient is put on heart lung machine by inserting pipes through the neck and the thigh. The heart is stopped by inserting the catheter retrogradely through the femoral artery in the upper part of the thigh up to the ascending aorta. The heart is stopped by inflating the balloon inside the aorta and giving potassium to temporarily stop the heart. The operation is done through a small cut in the side of the chest. Video assistance and shafted instruments help the surgeon to perform the surgery through small holes and fulfill the main goals of minimally invasive cardiac surgery, comfort, cosmesis, and fast rehabilitation. Voice activated video camera gives excellent view of the mitral valve. Port-access mitral valve surgery is a very important minimally invasive technique.
Surgical treatment of heart failure
Large number of heart patients develop and die from heart failure. Till recently most of these patients were managed with medicines without any surgical help. Recently lot of new surgical techniques have evolved to help treat patients with end stage heart failure. They include the Surgical Ventricular Restoration (SVR), Acorn procedure, Myosling, etc.
Left ventricular reconstructive surgery (dor procedure)
Left ventricle reconstructive surgery is a procedure sometimes used to treat heart failure. When a heart attack occurs in the left ventricle (left lower pumping chamber of the heart), a scar may form. The scared area can become thin and bulge out with each beat. The bulging thin area is called aneurysm. The aneurysm, along with the other damaged myocardium makes the heart to work harder to pump blood throughout the body. Initially the heart is able to handle the additional work, but over time the heart becomes larger than normal and pumps less effectively.
Left ventricular reconstructive surgery allows the removal of the scarred, dead area of the heart tissue and/or the aneurysm and return the left ventricle to a more normal shape. The goal is to improve heart failure and/or angina (chest pain) symptoms and possibly improve the pumping ability of the heart.
Other names of Left Ventricular Reconstructive Surgery:
- Endoventricular circular patch plasty repair
- Dor procedure (to credit Vincent Dor, MD, who authored many articles on the procedure he began performing in the early 1980s)
- Surgical Ventricular Restoration (SVR)
- Left ventricular infarct exclusion surgery
- Left ventricular aneurysmectomy reconstruction
- Surgical anterior ventricular endocardial restoration
Left ventricular reconstructive surgery is a major open-heart surgery, requiring the use of the heart-lung machine. The damaged part of the heart is removed and it is reconstructed with an artificial patch.
In addition to this procedure, coronary artery bypass graft (CABG) surgery is often performed to improve blood supply to the heart muscle. Further, about half of the patients undergoing the left ventricular reconstructive surgery, mitral valve leaks are also repaired.
Some patients may require a special device called an automatic implantable cardioverter-defibrillator (AICD) to treat serious abnormal heart rhythm, which is a very common postoperative problem in this type of procedure. Under special circumstances, an EP study (electrophysiology study) will have to be done to evaluate the heart rhythm.
Cardiac wrap surgery
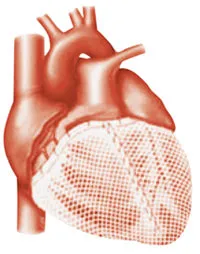
This procedure uses a technique that wraps the heart in a mesh bag, helping to prevent further enlargement and failure. A mesh wrap is pulled over the base of the heart and is attached with stitches. The goal is to prevent a weakened heart from enlarging (dilating) and failing further. Initial results are very encouraging and it is hoped that in a few years these procedures will be routinely offered to patients with heart failure.
Enhanced External Counterpulsation (EECP)
This is a non invasive techniqe. Inflatable pressure cuffs are placed on the calves, thighs and buttocks. These cuffs are in-flated and deflated in sync with the heartbeat. This increases the blood flow back to the heart
Arificial Heart
Although the heart is conceptually a simple organ (basically a muscle that functions as a pump), it embodies complex subtelities that defy straightforward emulation using synthetic materials and power supplies. The obvious benefit of a functional artificial heart would be to lower the need for heart transplants.
The total artificial heart (TAH) was first used in 1969 for a patient who was waiting for heart transplantation. An artificial heart is a prosthetic device that is implanted into the body to replace the original biological heart. It is distinct from a cardiac pump, which is an external device used to provide the functions of both the heart and the lungs. Thus, the cardiac pump need not be connected to both blood circuits. Also, a cardiac pump is only suitable for use not longer than a few hours, while for the artificial heart the current record is 17 months. Another problem is that an artificial heart requires an external power supply such as a battery pack worn on the patient’s waist; which carries a significant risk of introducing infection; no design so far has been able to use the body’s own natural biological energy. The first artificial heart patented was ‘Jarvik-7’, now known as Cardiowest C70 total artificial heart.
Robotic Cardiac Surgery
The next advance in heart surgery is the robotic surgery, which will revolutionise cardiothoracic procedures. Contrary to the popular belief, the robot does not do the surgery independently, rather the robot works as the extended arm of the surgeon. The surgeon sits on a computer control panel near the patient and controls the movement of various robotic arms. An assistant makes small holes in the patient’s chest wall through which the robotic arms are inserted.
The surgeon grasps and moves the highly sensitive instruments at the console while viewing the patient’s heart, greatly magnified on a screen. The robot precisely matches the surgeon’s natural hand and wrist movements, and translates them into precise, real time movements to the tiny instruments placed inside the patient through small puncture incisions. The procedure, for e.g., a mitral valve repair, will require three small incisions between the ribs, two for the insertion of interchangeable instruments and another for a thin, cylindrical video camera, called an endoscope.


There are many systems available, the most popular being da Vinci™ system.The da Vinci™ Surgical System provides the surgeon with the intuitive control, range of motion, fine tissue manipulation capability and 3-D visualization characteristic of open heart surgery, while simultaneously allowing the surgeon to work through small ports of a minimally invasive surgery. The patients experience shorter incisions, less pain and trauma and a quicker recovery time.
Stem Cell Therapy
Stem cells have the ability to grow into other types of cells and thus represent great promise for treating a wide range of diseases. While harvesting of embryonic (fetal) stem cells is extremely controversial, the cells used in the heart study came from the patient’s own bone marrow. Injected into the heart muscle, the stem cells developed into muscle and blood vessels in the damaged areas, increasing the heart’s pumping capability and blood flow. Using the patient’s own stem cells also eliminates the problem of rejection of donated cells and organs.
Total arterial revascularisation
In this procedure, coronary artery bypass graft surgery is done using all arterial grafts. Vein grafts are very rarely used. The various arterial conduits are the Internal Mammary Arteries, Radial artery, Gastroepiploic artery, and Inferior epigastric artery. The arterial grafts have longer patency rates unlike the vein grafts which start degenerating after 8 to 10 years, thereby necessitating the need for a second time (re-do) CABG.
Asian Heart Institute has been doing almost all total arterial revascularisation with excellent patency rates.
Valve repair surgery
Prosthetic valves came as a boon to patients with valvular heart disease, but with it came a new set of prosthesis-related problems. Awareness of these problems has refocused attention on developing techniques to preserve the patients narive valve. Surgeons developed renewed interest in reparative techniques to preserve mitral valve and devised methods to debride and reconstruct aortic valve.

