Early Detection of Asymptomatic Coronary Artery Disease in the Hospital Setting Using CT Imaging

CT coronary artery calcium scoring is guideline indicated for almost 50% of the adult population. However, this lifesaving technology that allows for the early detection of CAD is vastly underutilised worldwide. A formalised scientific programmatic approach can increase utilisation and deliver significant clinical and economic results.
For 50% of adults worldwide, the first symptom or warning of heart disease will be a heart attack or death. Despite the best of intentions, cardiology, imaging, and healthcare systems are not accurately identifying these vulnerable patients in a widespread manner until it is often too late. The most vulnerable demographic includes adults that fall into the “intermediate risk” category (ASCVD 7.5%-20% 10-year risk or males 45+ females 55+ years of age) defined by cardiovascular event risk prediction algorithms. The diminished predictive strength among this risk cohort exists because predictive models have a higher accuracy rate among the more predictable low-risk and high-risk cohorts but lack the same efficacy among the large segment of patients categorised as “intermediate risk.” To further illustrate the population health opportunity, consider that approximately 45% of adults fall into this largest intermediate risk designation and therefore remain underserved and vulnerable.
Prior to Cardiac CT imaging, including Coronary Artery Calcium Scoring (CAC), healthcare providers were limited to risk algorithm reliance and risk management until the presentation of symptoms allowed for diagnostic imaging to be employed. This left the largest risk cohort exposed, as, for 50%, a major coronary event would likely be that first symptom. With the genesis of CT based CAC testing availability, providers can now obtain a non-invasive diagnostic scan of the coronary arteries using this five minute test. The test utilises relatively new software that detects and quantifies calcified plaque in the arteries of the heart. The CAC study allows for an unequivocal diagnosis or rule-out of atherosclerotic disease and significantly changes the clinical paradigm, allowing an enhanced opportunity for heart attack prevention and a corresponding reduction in the number of preventable deaths. In many regions the test is being referred to as the “Mammogram of the Heart.”
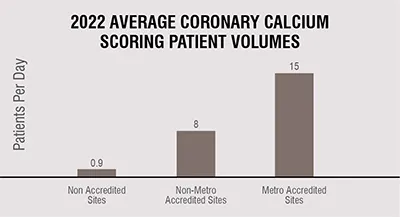
While published cardiovascular risk and prevention guidelines such as ACC, AHA, SHAPE, and ESC suggest almost 45% of adults would benefit from CAC scoring, hospitals today average less than one patient per day being tested (U= 3.5/week). CT CAC scoring is vastly underutilised, non-invasive, and is definitive for disease identification. Most hospitals in developed regions have invested in the technology and offer this diagnostic/preventive service, but lack patient volumes mirroring the Guideline suggestions. This equates to healthcare systems missing clinical opportunities for preventing heart attacks and growing the cardiovascular, imaging, and population health service lines.
Hospital underperformance is typically due to the absence of a focused programmatic approach, comprehensive primary provider training, and ongoing quality data acquisition and analysis to foster clinical and economic improvement.
CAC scoring outcomes data from over 150 hospitals in 16 countries, and over 350,000 CAC cases in the International Heart Attack Prevention Database https://nationalhearthealth.org/heart-attack-database suggest increased utilisation and referral patterns will afford an efficacious heat attack prevention strategy that has the potential to change the paradigm of atherosclerotic disease worldwide. The patient population that this technology will benefit most has been well defined and is well published. Increased adoption and utilisation will be largely determined by healthcare systems prioritising this technology and formalising patient selection/referral and medical management training to the front-line medical provider community.

The International Heart Health programme performed CT CAC testing on 350,142 asymptomatic patients (mean age 56.4), without known CAD, and classified “intermediate risk,” using the Framingham, ASCVD, or SCORE algorithms, between 2012-2022 in 151 medical facilities around the world. The CT CAC results were acquired using multi-slice CT scanners of at least 16 slice technology. No contrast was necessary for CT Calcium scoring procedures and the average testing time was less than five minutes in the scanner.
Traditional cardiovascular risk factors among tested patients included hypertension, elevated LDL cholesterol, diabetes, family history, tobacco use, and obesity. The most prominent risk factors that correlated best with increased disease incidence via CT calcium scoring were as follows: family history of CAD, elevated LDL cholesterol, and diabetes. Included patients averaged 3.1 risk factors in this worldwide cohort.
Calcium scoring outcomes/results include the following cardiovascular event risk categories and are based upon “Total Agatston Value” as determined by the presence or absence of detected calcification within the coronary arteries.

Accredited programme sites identified 213,581 asymptomatic patients (61%) with dae novo coronary artery disease using CT calcium scoring. Significantly, 18.2% (n=63,724) of patients tested were found to have “likely obstructive coronary artery disease” based upon a Calcium score of >400 Agatston value and were referred to cardiology for further testing and improved and more aggressive medical management. Scores exceeding 1000 are indicative of critical levels, often associated with the presence of at least one substantial blockage in a coronary artery. Participating sites identified 12,949 patients (3.7%) with these life-threatening scores and a majority went on for stent or CABG surgeries. The number needed to diagnose (NND) a patient having obstructive CAD was only six, and to identify at least one vessel critical stenosis was only 28, confirming the population health efficacy of this diagnostic test.
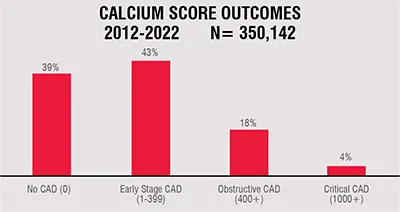
Importantly, participating hospitals reclassified 136,561 patients (39%) to “low risk” based upon a zero (0) calcium score. Evidence suggests these patients are at extremely low risk of a major coronary event (less than 1%) for the next five years and the need for further short-term evaluation and therapy are currently being debated.
Mean radiation exposure for coronary calcium scoring procedures was 1.01 mSv, which is patient friendly and comparable to mammography which has been used worldwide for decades with cost-benefit ratio widely accepted.
The economic impact at accredited sites was similarly impressive for both the CT imaging department and the cardiovascular service line. The implementation of a guideline based and accredited CAC scoring programme increased referrals and overall utilisation significantly from less than 1 patient/day to over 10 patients/day on average. Corresponding revenue averaged $311,550 annually in imaging department increases and $926,600 annually in cardiovascular service revenue gains.
Adoption of an evidence based, and guideline supported CT coronary calcium scoring programme can promote early detection and treatment, and thus change the paradigm of cardiovascular disease, reduce major coronary events, and enhance the cardiovascular service and imaging lines of healthcare providers as we advance worldwide toward lower cost, non-invasive testing for chronic disease. Clinical outcomes data is remarkably similar across countries and even continents as this test becomes increasingly entrenched in the standard of care across the Western world. The opportunity to change the paradigm of cardiovascular disease and its debilitating effects across populations and reduce healthcare expenditures globally is now.

