Cerebral Small Vessel Disease Burden is Associated with Outcomes after Minimally Invasive Surgery of Acute Spontaneous Intracerebral Haemorrhage

This pre-specified sub study of data from the MISTIE III trial investigating the association between cerebral small vessel disease (CSVD) features on MRI and therapeutic outcomes of minimally invasive surgery in patients with acute spontaneous supratentorial intracerebral haemorrhage. Main findings showed that CSVD burden is associated with functional outcomes in those with successful haematoma reduction (end of treatment ICH volume ≤15 mL).
Cerebral small vessel disease (CSVD) comprises clinical, neuroimaging and pathological findings involving the small penetrating vessels of the brain. CSVD has been linked to cognitive dysfunction and is both a risk factor for spontaneous intracerebral haemorrhage (ICH) as well as a predictor of poor functional outcomes after ICH occurrence. (1) In particular, brain imaging biomarkers of CSVD, such as white matter hyperintensities (WMH), cerebral microbleeds (CMBs), or superficial siderosis (cSS), are associated with a higher risk of intracerebral haemorrhage (ICH) recurrence, and with poor outcomes in predominantly lobar hemorrhages. (1,2)
There are few proven therapies for spontaneous ICH and although minimally invasive surgery (MIS) is being intensely studied, the definitive efficacy of surgical haematoma removal remains controversial, including specific patient groups who may benefit the most.
This study (3) was a pre-specified subgroup analysis in which we investigated whether cerebral small vessel disease is associated with functional outcomes after MIS for spontaneous ICH as performed in the Minimally Invasive Surgery Plus Alteplase for Intracerebral Haemorrhage Evacuation (MISTIE III) trial (4), the first clinical trial of stereotactic thrombolysis for spontaneous ICH to define thresholds for potential benefit from clot volume reduction. MISTIE III was neutral for the primary outcome of modified Rankin Score (mRS) 0-3 at one year follow-up comparing patients treated with MIS vs. standard medical care (SMC). However, the subgroup of patients with successful surgery (reaching the pre-specified end of treatment (EOT) volume of <15 mL) experienced a significant improvement in good outcomes compared with SMC. This group was therefore of primary interest to the current study.
We defined CSVD using five well-described CSVD features according to the STRIVE consensus (5): lacunar infarcts, white matter hyperintensities (WMHs), enlarged peri-vascular spaces (EPVS), cerebral microbleeds (CMBs), and cortical superficial siderosis (cSS). We also analysed this data using 3 grading tools: the CSVD burden score (6), the Cerebral Amyloid Angiopathy (CAA) score (7), and a modified CSVD (mCSVD) score which we developed based on the distribution of CSVD features in our cohort. The cohort consisted of 288 patients who had at least one MRI (performed at a median of 1 day after ICH onset), and full clinical data.
In the MISTIE III trial cohort, which included only patients with good baseline function (mRS 0-1), but with large ICH (>30 mL) we found a high proportion of CSVD imaging findings on the baseline MRI. Using modified Boston criteria (8) 61% of this severe ICH cohort had “possible CAA,” and 18% met criteria for “probable CAA.” These CSVD findings including all 3 compositae scores were almost all (with exception of EPVS in the basal ganglia) significantly associated with poor outcome at 1 year in the surgical group. In the SMC group, none of these MRI features were associated with poor outcome after adjustment for other covariates.
Comparing the SMC group to MIS patients with successful surgery (EOT volume <15 mL), we found that presence of lacunes, severe white matter hyperintensities and CAA score>1 significantly modified one-year outcomes in the MIS group in favour of lower odds of a poor outcome when these MRI findings were absent. Stated another way, successful haematoma reduction by MIS was associated with significantly lower odds of good functional outcome when patients had a higher total burden of CSVD, and particularly presence of lacunes and severe WMHs. Comparing all MIS to SMC patients, we did not find any significant heterogeneity in the effect of MIS on one-year outcomes by any specific CSVD feature or by CSVD scores.
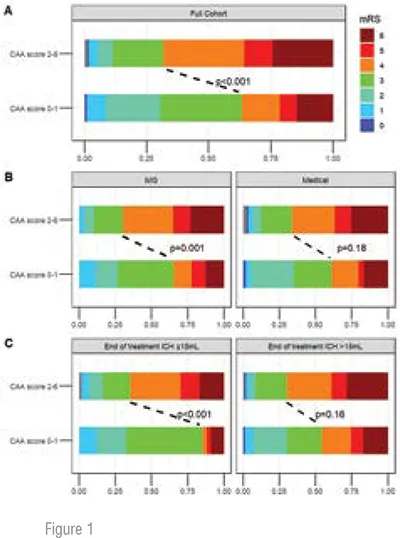
Figure 1 shows mRS score distribution by CAA score 0–1 versus 2–6 in (A) full MRI cohort (n=288), (B) MIS (n=149) versus medical (n=139) groups and (C) EOT volume≤15 mL (n=94) versus>15 mL (n=194). This figure shows that the odds of a good outcome (mRS 0–3 vs 4–6) were significantly higher for patients with CAA score 0–1 (vs 2–6) in fully adjusted analyses for the full cohort, MIS group and group with EOT volume ≤15 mL, but not for the SMC group and group with EOT volume>15 mL.
These findings emphasise the importance of substantial haematoma volume reduction when performing MIS for ICH, and the clinical implications of pre-existing small vessel disease in defining long-term outcomes even after successful clot evacuation.
The specific MRI features of greatest importance, lacunes and WMHs are both markers of cerebral ischaemia and are associated with severity of hypertension and with cognitive decline in older people (9, 10). Therefore, chronic vascular dysfunction may be an important pre-existing condition which limits good outcomes after surgical treatment of ICH. Alternatively, these ischaemic markers may portend new conditions that limit recovery such as post stroke depression, cognitive impairment, and new ischaemic strokes, all of which are associated with white matter hyperintensities (11-14).
This data is consistent with the ischaemic stroke literature showing the relationship between CSVD markers and the outcomes of mechanical thrombectomy for large vessel occlusion, where severe WMH and higher CSVD scores have been correlated with poor 90-day outcomes (15). These data and ours highlight the current interest in identifying patients most suitable for interventional treatments to increase rates of good prognosis.
This was an exploratory study and has both strengths and limitations. MISTIE III was a well adjudicated clinical trial with blinded outcomes and a core of trained imaging reviewers blinded to clinical information. Weaknesses include generalisability where MISTIE III was very selective and specifically excluded patients with baseline mRS >1, ICH volume <30 mL, and clinical herniation. The trial was conducted in tertiary care academic settings which may not represent medical care in a community setting. Finally, MRI was difficult to obtain in high severity ICH patients limiting the number of available studies which may have biased our sample although baseline ICH volume, Glasgow Coma Scale and outcomes were not different between participants with and without MRI. More sophisticated MRI analysis including volumetric analysis of WMH and diffusion tensor imaging analysis of integrity of white matter tracts are areas for future research.
As the first study to evaluate use of MRI to target surgical therapy to those most likely to benefit, we do not currently recommend utilisation of CSVD features or CSVD scores as selection criteria for MIS for ICH. Rather these findings may help to stratify or select patients for clinical trials for ICH interventions where such imaging is available.
References:
1. Lioutas VA, Wu B, Norton C, Helenius J, Modak J, Selim M. Cerebral small vessel disease burden and functional and radiographic outcomes in intracerebral hemorrhage. J Neurol. 2018;265(12):2803-2814.
2. Sato S, Delcourt C, Heeley E, et al. Significance of Cerebral Small-Vessel Disease in Acute Intracerebral Hemorrhage. Stroke 2016;47:701-707.
3. Wardlaw JM, Smith EE, Biessels GJ, et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol 2013;12:822-838.
4. Li Y, Cho SM, Avadhani R, Ali H, Hao Y, Murthy SB, Goldstein JN, Xia F, Hu X, Ullman NL, Awad I, Hanley D, Ziai WC. Cerebral small vessel disease modifies outcomes after minimally invasive surgery for intracerebral haemorrhage. Stroke Vasc Neurol. 2023 Nov 10:svn-2023-002463.
5. Hanley DF, Thompson RE, Rosenblum M, et al. Efficacy and safety of minimally invasive surgery with thrombolysis in intracerebral haemorrhage evacuation (MISTIE III): a randomised, controlled, open-label, blinded endpoint phase 3 trial. Lancet 2019;393:1021-1032.
6. Staals J, Makin SDJ, Doubal FN, et al. Stroke subtype, vascular risk factors, and total MRI brain small-vessel disease burden. Neurology 2014;83:1228-34.
7. Charidimou A, Martinez-Ramirez S, Reijmer YD, et al. Total magnetic resonance imaging burden of small vessel disease in cerebral amyloid angiopathy an imaging-pathologic study of concept validation. JAMA Neurol 2016;73:994-1001.
8. Fazekas F, Barkhof F, Wahlund LO, et al. CT and MRI rating of white matter lesions. Cerebrovasc Dis 2002;13 Suppl 2:31–6.
9. Wardlaw JM, Smith EE, Biessels GJ, et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol 2013;12:822–38.
10. Liang Y, Chen Y-K, Mok VC-T, et al. Cerebral small vessel disease burden is associated with poststroke depressive symptoms: a 15-month prospective study. Front Aging Neurosci 2018;10:46.
11. Georgakis MK, Duering M, Wardlaw JM, et al. WMH and long-term outcomes in ischemic stroke: a systematic review and meta-analysis. Neurology 2019;92:e1298–308.
12. Shi L, Zhao L, Yeung FK, et al. Mapping the contribution and strategic distribution patterns of neuroimaging features of small vessel disease in poststroke cognitive impairment. J Neurol Neurosurg Psychiatry 2018;89:918–26.
13. Ryu W-S, Schellingerhout D, Hong K-S, et al. White matter hyperintensity load on stroke recurrence and mortality at 1 year after ischemic stroke. Neurology 2019;93:e578–89.
14. Uniken Venema SM, Postma AA, van den Wijngaard IR, et al. White matter lesions and outcomes after endovascular treatment for acute ischemic stroke: MR CLEAN Registry results. Stroke 2021;52:2849–57.
15. Fan R, Gan J, Chen F, Le C, Chen Y. Overall cerebral small vessel disease burden is associated with outcome of acute ischemic stroke after mechanical thrombectomy. Interv Neuroradiol. 2022 Nov 9:15910199221138140.

