Innovations for Providing Minimally Invasive Surgeries in Rural Areas
Frugal Equipment, VRiMS & Robotic Arm

This article explores innovative approaches to improve access to Minimally Invasive Surgeries (MIS) in rural areas through frugal and digital technologies. Utilizing the Gas Insufflation Less Laparoscopic Surgery (GILLS) system, laptop cystoscope and virtual reality training, these methods empower local surgeons and enhance healthcare delivery in underserved communities.
Minimally Invasive Surgeries (MIS) offer significant advantages in rural and remote areas, as they utilize limited resources effectively, reduce travel for patients and their families, and minimize the carbon footprint. However, challenges such as high equipment costs and limited training programs hinder widespread implementation.
Our experience shows that innovative partnerships among mission hospitals, churches, mission organizations, and overseas consultants can enhance surgical care in these underserved communities. While previous short-term medical missions often struggled due to a lack of long-term vision, integrating frugal innovations into strategic partnerships can create sustainable, win-win solutions for all involved. In this proposal, we will outline our findings related to frugal and digital innovations that successfully facilitate access to MIS in rural areas.
We realize that effective education for surgeons in these settings is critical for improving access to surgical care. This article outlines our approach, experiences, and the potential impact of this initiative on surgical training and outcomes in underserved populations.
THE PROBLEMS / NEED
Access to safe surgical care remains a critical unmet need globally, with approximately five billion people lacking access, particularly in low- and middle-income countries (LMICs). The Lancet Commission on Global Surgery estimates that a population of 100,000 ideally requires 5,000 surgical procedures annually, yet in India, the average is merely 800 procedures, with rural areas recording as few as 30 to 300 surgeries per year.
The challenges of conventional surgical training are evident, particularly in rural areas where healthcare providers are required to leave their communities for education in urban centers. This relocation incurs significant financial burdens related to travel, living expenses, and training fees, discouraging aspiring surgeons. Additionally, when trainee surgeons depart from rural facilities, the existing hospitals suffer from a shortage of skilled personnel, further diminishing their ability to provide essential surgical services.
THE FRUGAL INNOVATIONS
There are two frugal innovations that helped us to take MIS to rural areas. Both these are included in the WHO Compendium of innovative medical technologies for low resource limited setting.
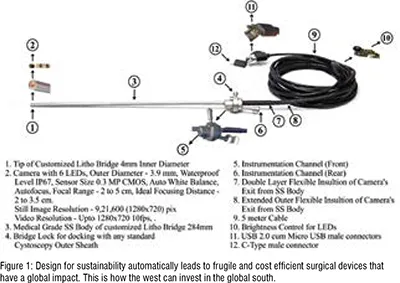
The first one is the Laptop Cystoscope which is a plug and play device that is used for diagnostic cystoscopies and minor procedures instead of the conventional cystoscope that needs the expensive telescope, camera, light source, monitor, etc., thereby reducing the investment needed to about 5 to 10% of the conventional cystoscopes.
The other device is the Gas Insufflation Less Laparoscopic Surgeries [GILLS] device that mechanically elevates the abdominal wall for laparoscopic surgeries thus making laparoscopic surgeries possible under the low – cost and safe Spinal Anaesthesia.

THE PROCESS INNOVATIONS
The model of Diagnostic Camps followed by surgical camps were used in rural areas because only 25% of the patients knew that they had surgically treatable conditions before the Diagnostic Camps in rural areas.
These surgical camps were used for training and empowerment of the local rural surgeons. Formal training programs involving Proctorship at the trainee’s place was developed with the help of University of Leeds project.
THE OPPORTUNITY
Minimally Invasive Surgeries (MIS) present a unique opportunity to significantly increase surgical coverage in rural regions. Studies have shown that the implementation of laparoscopic techniques can boost surgical rates to 800–1,200 procedures per 100,000 population annually. These minimally invasive procedures utilize limited resources efficiently, allowing patients and their families to reduce both travel time and expenses while lowering the carbon footprint associated with surgeries.
PROPOSED SOLUTION
Empowering rural surgeons to perform MIS is the way forward in meeting the needs of rural surgical patients. Seed project funded by the German Hospital Partnership program carried out with the DTC (German Global Surgery Association) empowered 18 rural hospitals in India training the local surgeons to perform MIS using the Gas Insufflation Laparoscopic Surgeries and laptop cystoscope for endoscopic urology surgeries increased the number of surgical procedures carried out at these hospitals from 1844 to 6363 after empowerment which increased the surgical coverage rate in the target population from 580 to 2148 per 100000 / year after empowerment.

CONVENTIONAL SURGICAL TRAINING
Conventional training often requires rural surgeons to relocate to urban facilities, which can be costly. Traditional methods focus heavily on observation, making it difficult for trainees to fully understand surgical procedures from their positions in crowded operating rooms. This limitation leads to missed learning opportunities and slows skill development. Additionally, hands-on training can be both slow and risky since trainees might have to operate on live patients without enough practice. After completing their training, these surgeons often find it hard to access resources for ongoing education and skill improvement in their rural settings, adding to their challenges.
THE DIGITAL TECHNOLOGIES
The Virtual Reality in Medicine and Surgery [VRiMS] has helped with training from a remote location after short contact training program. It involves 360 camera and inlays from the monitor feeds, close view camera and other teaching feeds. The trainees can observe surgical procedures virtually (at the best possible position in the Operating Room next to the surgeon).
The use of virtual reality for training allows for self-paced learning without the need for relocation, giving surgeons the chance to hone their skills in their own environments. Trainees will practice using lifelike simulators to develop proficiency in surgical skills such as suturing and instrument handling.
REFERENCES
1. Jesudian Gnanaraj, Michael Rhodes. Surgical work in Medial Missions. A study in remote areas of India. Christian Journal for Global Health. 1(2): 42-47. Nov 2014
2. Grundmann GH. Mission and healing in historical perspective. Int B of Mission Research. 2008;32(4):185-8. http://dx.doi.org/10.1177/239693930803200404
3. Gnanaraj J. Working Holidays for Overseas Doctors: Host Perspective in Mission Hospitals in Rural India. Christian Journal for Global Health (May 2015), 2(1):35-42
4. Gnanaraj J, Gnanaraj K, Islary B, Sumi B, Mathew G. Frugal innovations that helped mission hospitals manage during the pandemic and further suggestions. Christ J for Global Health. November 2020; 7( 4):33-38. https://doi.org/10.15566/cjgh.v7i4.419
5. Gnanaraj Jesudian. Empowering the Rural Surgeons, the way forward for meeting the surgical needs of Rural Areas. doi: 10.52648/JoGS.1136
6. Gnanaraj J, Gnanaraj K, Islary B, Sumi B, Mathew G. Frugal innovations that helped mission hospitals manage during the pandemic and further suggestions. Christ J for Global Health. November 2020; 7( 4):33-38. https://doi.org/10.15566/cjgh.v7i4.419
7. J. Gnanaraj, Lau Xe Xiang Jason, Hanah Khiangte. High quality surgical care at low cost: The Diagnostic camp model of Burrows Memorial Christian Hospital. Indian Journal of Surgery Vol. 69, No.6, December 2007 p 243-247
8. Aruparayil N, Gnanaraj J, Maiti S, Chauhan M, Quyn A, Mishra A, Bains L, Mathew G, Harris C, Cundill B, Fellows A, Gordon K, Dawkins B, Shinkins B, Brown J, Jayne D. Training programme in gasless laparoscopy for rural surgeons of India (TARGET study) - Observational feasibility study. Int J Surg Open. 2021 Sep;35:None. doi: 10.1016/j.ijso.2021.100399.
9. Atul Ranjan Mallik, Gnanaraj Jesudian, Henning Mothes. Analysis Of the Impact Of GILLS (Gas Insufflation-less Laparoscopic Surgery) In Selected Rural Hospitals In India. doi: 10.52648/JoGS.1186
10. Available from: https://www.vrims.net/post/gills-surgery-training-and-vr-kabale-university (accessed on December 20, 2024)
11. Available from: https://www.proximie.com/

