Patient-Physician Communication by Using Mobile Technology in Developing Countries




The positive outcomes of a successful patient-physician communication are widespread considering the health related aspects. The rapid proliferation of mobile technology has facilitated the healthcare system to provide better support and establish sustainable implication of standard procedures in a broader range of healthcare services.
Patient-Physician communication is one of the foremost important part in patient care, given the godlike stature of physicians in many countries. This is critical for every physician to deliver a high-quality healthcare. Patient health outcomes depend on effective communication with the physician. Many physicians encourage open communication and complete information for getting more accurate diagnosis, proper counselling, improving treatment plans and better health outcome.
The Institute of Medicine (IoM), allied with American College of Obstetricians and Gynecologists, has identified the use of information and communication technology (ICT) as one of the perilous forces obligatory for improving the quality of healthcare in the developed countries. Currently, more physicians are becoming handy in using mobile health technology for keeping health records and web messaging to communicate with their patients. The South-East Asia region still has some barriers to implement mobile health technology including policy, technical knowledge and expertise and service costs for implementation of such services. To make mobile healthcare technology more effective and user friendly, our understanding is, that it is essential to improve the way of implementation from top to bottom.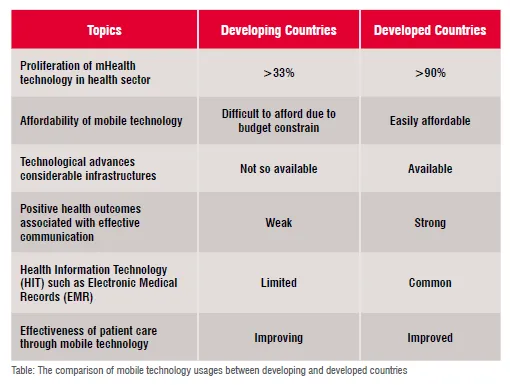
Despite of fragile infrastructure, in developing countries, telecommunication technologies are heading towards a ground-breaking platform rapidly for the last couple of years. Consequently, it has already created an ample of scopes to develop and utilise this technology in patient-physician communications. Easy accessibility, reasonable expenses of the mobile phone, catchy advertisement and different types of tariff services enable mass acceptance among the consumers unlike with some other technologies. The service providers introduce their value-added services (VAS) through the integration of healthcare for those people who live in comparatively remote areas of the country. This article presents issues focused on patient-physician communication in the context of a fast-developing country, Bangladesh.
Serious health challenges like non-communicable diseases are hindered by several core impediments; among them a universal scarcity of healthcare workers. According to the WHO, there is a perilous shortfall in healthcare workers, in lieu of a total deficit of 2.4 million healthcare workers worldwide and among the 57 countries, mostly in the developing countries. This human resources constraint intensifies the already increasing pressure on developing countries’ health systems. To cope with the burden of containing the spread of non-communicable diseases (NCDs), governments, businesses, NGOs, foundations, and multilateral organisations all recognise the importance of leveraging new tools and solutions to address these distinct but interrelated health challenges.
In the meantime, mobile communication offers an effective means of bringing healthcare services to developing countries with low-cost handsets and the penetration of mobile phone networks globally. Tens of millions of people that never had consistent access to a fixed-line telephone or computer now use mobile devices as daily tools for communication and data transfer. Now, a full 64 per cent of all mobile phone users can be found in the developing countries. Furthermore, estimates show that half of all individuals in remote areas of the developing countries use mobile phones. This growing ubiquity of mobile phones is a vibrant element in the aptitude of mobile technologies for health.
Furthermore, greater emphasis on patient-centred care could improve communication between doctors and patients in developing countries and increase the effectiveness of care so that it can be as competent as developed countries. The penetration of mHealth is more than 90 percent in the developed world and 33 percent in the developing world. South Asian countries like Bangladesh adopt appropriate initiatives. in the development of Electronic Medical Records (EMRs) to fulfill their specific necessities. Technological advances often need substantial infrastructure investment in electricity, computer equipment, and telephone/internet networks; but in developing countries healthcare budgets are also inadequate and strained. Moreover, depending on the obtainability of time and the patient load, managing EMR during care delivery has been a cumbersome process for the clinicians, particularly in the developing countries where the doctor-patient ratio is much worse than in developed countries. However, developing countries, with their less extensive healthcare infrastructure, would benefit the most from mobile health (see Table).
 Due to the existing diversified opinions regarding mobile phone technology services and usage, it has an optimistic impression on patient healthcare. The ongoing practice shows that the physicians provide paper-based prescription for detailing patient grievances. Moreover, you will find a completely different scenario where the doctor-patient ratio is very low and the physicians almost perpetually have to work in a time-constrained fashion. Using mobile technology in such a situation could be problematic. This paper, however, mainly pointed the patient-physician common practice of health care-related information, storage and uses as well as develop communication in such a setup.
Due to the existing diversified opinions regarding mobile phone technology services and usage, it has an optimistic impression on patient healthcare. The ongoing practice shows that the physicians provide paper-based prescription for detailing patient grievances. Moreover, you will find a completely different scenario where the doctor-patient ratio is very low and the physicians almost perpetually have to work in a time-constrained fashion. Using mobile technology in such a situation could be problematic. This paper, however, mainly pointed the patient-physician common practice of health care-related information, storage and uses as well as develop communication in such a setup.
Healthcare services delivered through mobile phonein developing countries like Bangladesh, are becoming popular both in urban and remote rural areas due to the significant shortage of highly trained healthcare personnel, and expenses. For example, Grameen phone (GP), the largest network coverage mobile phone company in Bangladesh, covers over 98 percent of the total population and over 87 percent of the land area for providing healthcare services through mobile phone. Even though the service is playing a vital role, unfortunately, lack of tele-health education, proficient manpower, and frequent monitoring by the physicians are hindering the process.
In Bangladesh, Grameen’s mobile phone created a “HealthLine” where anyone can call a mobile hotline and consult a doctor on 24/7 basis. More than two million people, mostly women, use the system each year from the remotest part of the country. That apart, there is “Aponjon”, a brand of mHealth service through mobile phones for expecting and new mothers in Bangladesh under the auspices of Mobile Alliance for Maternal Action (MAMA). Another service called “Healthlink” was launched by Banglalink for its customers to provide innovative and convenient health services.
The usability of mobile health systems is a key factor in the acceptance and diffusion of such technology in disease management and wellness promotion. In this context, four factors need to be addressed: user-friendliness, usability, user competence, and confidence. The first two factors deal mostly with the type of mobile technology (hardware matters such as size, noise, aesthetic presence, and obtrusiveness, and software matters such as user interfaces and device operation), whereas the last two factors relate more to users and their perceptions.
Mobile technology services seek to increase access to between-visit support by augmenting clinician contact with automated services delivered via smart/feature phones, short message service (SMS), and interactive voice response (IVR). Recently, the strategy for improving outcomes of people with noncommunicable diseases (NCDs) has been widely-accepted through tele-health management. For instance, linking the hypertensive patients and home-based blood pressure (BP) monitoring with telehealth follow-up service creates effective outcome. Therefore, automated mobile phone management and behavior-change calls can improve self-care as well as health outcomes among NCD patients and may be more cost-effective than in-person visits.
Among the NCDs, hypertension is an increasing problem in Southeast Asia, particularly in Bangladesh. The statistics show that it is an emerging epidemic and prevalence was found within 15-20 per cent adults and 40-60 per cent among elderly people of Bangladesh. A common digital infrastructure can be used to generate the automated calls with the help of Bangladesh Telecommunication Regulatory Commission (BTRC) such as local telephone systems via session initiation protocol lines and voice over Internet protocol (VoIP) technology. Automated calls will use as tree-structured algorithm in order to gather information of the patient’s BP, self-monitoring BP, medication adherence, and diet (according to the World Health Organization) and to provide tailored advice based on the patient’s responses. Mobile tools can monitorpatient’s hypertension status, drug and diet adherence, and seeking laboratory investigations. SMS through mobile phone can be used as a two-way communication system between wired hypertensive individuals and healthcare providers. It will provide primary health education and BP measurement reminders to encourage adherence to medical advice. Hypertensive individuals will receive standard hypertensive healthcare services, and counselling as well as behavioural change educations over the mobile phone as a competent and effective way.
During the call, patients receive a reminder to check their BP regularly and are asked about recent systolic values, medication adherence, and intake of salty foods. Based on their reports, hypertensive individuals will receive additional self-care information and prompts to seek medical attention or medication refills to address unacceptably high or low BP. A structured e-mail alert for healthcare providers will be generated automatically once the patients report their health status. In addition, the patients will get reminders if they don’t report regularly or never take BP medications or when they have less than a 2-weeks supply.
Patients will have the option of enrolling with a family member or friend, who will receive a brief automated mobile update regarding the patient’s self-reported health status each week, including information about the patient’s hypertension self-care and how that caregiver could help the patient make their self-management more effective.
For accomplishing ‘Vision 2021’ milestones, Bangladesh government has executed e-health as an e-solution to the health sectors due to lack of accessibility of doctors as well as digital Bangladesh ingenuities. Mobile technology has been allied with every health sector especially for hospital healthcare providers; they used web cam and publicly accessible mobile phone for monitoring patient care. Physicians can unify videoconference and send advisory SMS such as vaccine alerts, medicine reminder plan, and pregnancy related suggestions to the patient. Electronic data are transferred into patient record and management.
In developing countries like Bangladesh, criticisms about doctors are often interrelated to issues of communication, not quantifiable aptitude. Every patientdesires that the physician may perhapsdexterously diagnose and treat their sicknesses and effortlessly communicate with them. Physicians with improved communication and interactive aids can identify difficulties earlier by using mobile technology. Moreover, it can avert medical emergencies and intervention, afford better provision to their patients and begin sustainable superlative practices in a broad range of healthcare services.
Finally, the explanation provided here can be executed for a developing country to trial in a multi-care setup that treats NCD patients. Nevertheless, in the Bangladesh context, physician-patient ratio is average 1:2000 and the solution can be implemented in a setup where physicians have to manage a huge number of patients. Moreover, they need to document all patient-related information manually and have no inter-legislative connection for patient information sharing response, when it comes to abridging the total procedure by using mobile phone technology.
References:
01. http://www.banglajol.info/index.php/BMJ/article/viewFile/18786/13131
02. www.banglajol.info/index.php/NIMCJ/article/download/23169/15946
03. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3096184/
04. http://www.ijogr.com/blog/2015/patient-doctor-communication
05. http://annals.org/aim/article/711682/electronic-patient-physician-communication-problems-promise
06. http://www.daily-sun.com/printversion/details/151556/Doctorpatient-relationship:-An-untouched-issue-in-Bangladesh
07. www.atlantis-press.com/php/download_paper.php?id=13590
08. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4297607/
09. http://www.healthcare-informatics.com/news-item/survey-doctors-and-patients-see-benefits-mobile-apps
10. http://ci-journal.net/index.php/ciej/article/view/941/1011
11. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3880062/
12. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4800908/
13. https://dash.harvard.edu/bitstream/handle/1/3382980/Mandl_Electronic.pdf
14. https://www.telenor.com/wp-content/uploads/2012/05/BCG-Telenor-Mobile-Health-Report-May-20121.pdf
15. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1496871/
16. http://www.ehealth-connection.org/files/conf-materials/mHealth
17. http://content.healthaffairs.org/content/29/2/252.full
18. http://who.int/pmnch/about/steering_committee/board8_preboardpresentation_chowdhury.pdf
19. https://www.theguardian.com/sustainable-business/technology-mobile-health-developing-countries
20. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5114432/
21. http://www.globalproblems-globalsolutions-files.org/unf_website/assets/publications/technology/mhealth/mHealth_for_Development_full.pdf

