Pre-Hospital Delay in Stroke Care in India: The Importance of Location and Distance from Specialty Centre-A Comparison of two locations
Delay during Stroke- Distance and Location
.webp)
This article highlights the critical global health issue of stroke, emphasizing the urgency of timely treatment to mitigate mortality and disability. Ischemic stroke, more prevalent than hemorrhagic stroke, demands swift intervention within the Golden Hours. Disparities in healthcare facilities, compounded by geographical challenges, significantly affect stroke care. A comparative study of two districts in Kerala underscores the pivotal role of location in timely treatment access, emphasizing the imperative for strategic solutions like enhanced referral centers, widespread health education, and a resilient emergency care network.
Introduction:
Stroke is responsible for a substantial proportion of mortality and disability across the globe. There are two types: Ischemic stroke and Hemorrhagic stroke. Ischemic stroke is more prevalent compared to hemorrhagic stroke. One of the crucial aspects of stroke treatment is time. Early treatment reception has been proven to reduce mortality and disability significantly. Also, the most common acute treatment for stroke is thrombolysis using pharmacological agents like ‘recombinant tissue plasminogen activator (rtPA).’ Thrombolysis for stroke is limited to 4.5 hours after the onset of symptoms of a stroke, and this time window is known as the Golden Hours. Delayed treatment seeking or arrival at the stroke center may lead to ineligibility to thrombolysis. This will cause severe disability or mortality to stroke victims. Globally, organizations like the American Stroke Association (ASA) are trying to increase awareness regarding stroke symptoms and treatment. The aim is to improve the percentage of stroke victims receiving Golden Hour treatments. However, various underlying factors like socio-economic factors, low awareness, unavailability, or accessibility to stroke treatment are causing hindrances to this goal. This article emphasizes the need to consider the distance and location of stroke centers in various regions. Meeting bed or health worker ratio based on population can create insufficiencies in stroke care because delays during transport due to distance or logistic issues can result in denial of Golden hour treatment.
In this article, we compare two districts in Kerala. to understand the need to consider distance and location in stroke care as significant factors. Kerala is a southern Indian state known for its achievements in healthcare and socio-cultural reforms. Kerala has been ranked top nationwide during repeated NITI Aayog health indexing assessments. Their achievements include the highest vaccination rate, literacy rate, gender equality, lowest maternal and infant mortality rate in the country, and many more. However, multiple past studies conducted in Kerala have shown the distance and location of stroke victims as a reason for delay. Also, studies show that a meager percentage of stroke victims in the state are receiving Golden Hour treatments for stroke. In this article, we compare two districts in Kerala to study the distribution of stroke care facilities and geographical matters crucial in the victims' decision-making and transport during a stroke.
Comparison of Two Districts:
Kerala is known for its geographical diversity, especially the vast coastal line, western Ghat mountains, and various hills, backwaters, and rivers across the state. However, this makes logistics difficult in many regions of heavily populated states. In this study, we are comparing two Districts, Ernakulum and Idukki. We considered these two districts because of their highly different geography, urbanization, and development status.
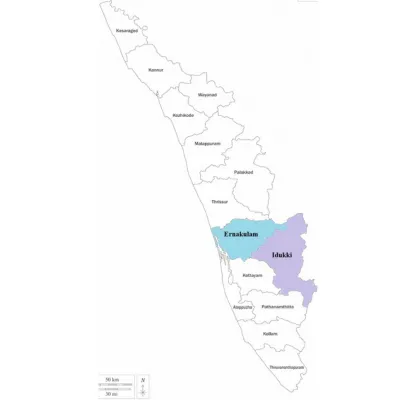
Figure 1: Map of Kerala showing the location of neighboring districts Ernakulum and Idukki
Geographic Diversity:
Ernakulum is almost wholly inhabited and a heavily urbanized district; however, neighboring Idukki is nearly 80% covered with dense forest and mountains. Ernakulum is low elevated from the sea level and well connected across the district through roads and a railway network. Most of the areas of Idukki are uninhabited, with remote locations where residents live. Most of these areas are connected by mountain roads, which are challenging to drive through, and the district needs Rail or Air connectivity.
Table 1: State Health Agency.
|
|
Public Hospitals – Ernakulum |
|
Public Hospitals – Idukki |
|
1 |
CHC Kalady |
1 |
District Hospital, Thodupuzha |
|
2 |
CHC Moothakunnam |
2 |
Govt: Medical College Hospital Idukki |
|
3 |
CHC Pandappilly |
3 |
THQ Hospital, Nedumkandam |
|
4 |
Cochin Cancer Research Centre |
4 |
Taluk Hospital Kattappana |
|
5 |
District Hospital Aluva |
5 |
THQ Hospital Adimali |
|
6 |
General Hospital, Muvattupuzha |
6 |
THQ Hospital Peermade |
|
7 |
General Hospital Ernakulum |
|
|
|
8 |
Govt. Maharaja’s Taluk Hospital |
|
|
|
9 |
Govt.Medical College,Ernakulam |
|
|
|
10 |
THQ Hospital, Perumbavoor |
|
|
|
11 |
Taluk Hospital Piravom |
|
|
|
12 |
Taluk Hospital Angamaly |
|
|
|
13 |
THQ Hospital Fortkochi |
|
|
|
14 |
THQ Hospital (CHC Kothamangalam) |
|
|
|
15 |
THQ Hospital N Paravur |
|
|
|
16 |
THQ Hospital Tripunithura |
|
|
|
17 |
W&C Hospital, Mattanchery |
|
|
*THQ: Taluk Head Quarters
Healthcare Establishments:
Ernakulum is a hub of public and private healthcare facilities. However, Idukki residents depend on neighboring districts for most of their specialty treatments. The population in Ernakulum is three times that of Idukki; hence, the need for hospital beds and health workers is also high. Also, as an urbanized district, many people from neighboring communities utilize Ernakulum’s healthcare facilities. 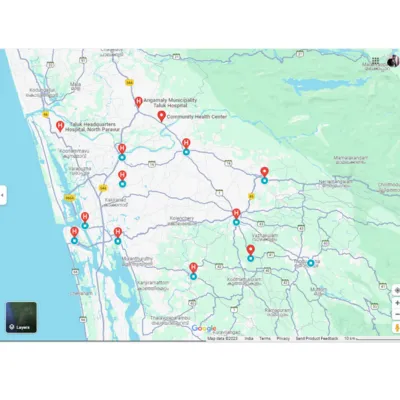
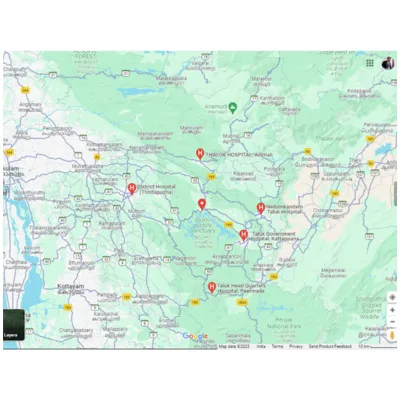
Figure.2 Ernakulum (Copyrights: Google Map Data ©2023) Figure.3 Idukki (Copyrights: Google Map Data ©2023)
Controversy of Location and Distance vs. Saturation of Bed and Health Worker Ratio in Stroke Care
Figure 2& 3 shows the distribution of public hospitals across the two districts. In Ernakulum, the number of hospitals is high and distributed across the entire district. On the contrary, the hospitals in Idukki are far from each other, and a vast area around each healthcare facility does not have any health facilities. The map shows dense forest lands and water bodies in Idukki; however, Ernakulum has more urbanized areas.
Idukki is much less populated than Ernakulum (340,0000 with a population projection of just above 100,0000 in 2023. This population disparity shows that healthcare requirements, including human resources, hospital beds, and other facilities, are much higher in Ernakulum. However, the controversy is the logistic aspects of stroke care. Travel time, availability of stroke care, and faster diagnosis and referral are very important. Scattered facilities and extended travel are barriers to stroke care.
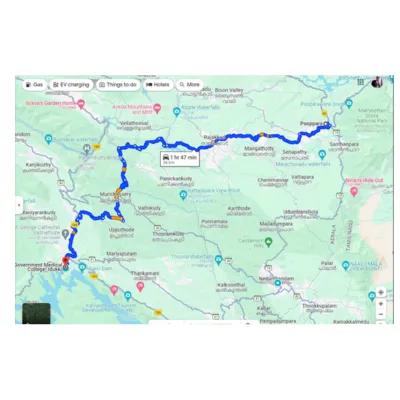
Figure.4: Distance from Pooppara to Idukki Medical College in Google Map (Copyrights: Google Map Data ©2023)
The distance from Poopparara, a remote residential location in Idukki, is around 50 km from the specialty treatment center, Idukki Medical College, with a travel time of around 2 hours. This is critical because delaying decisions due to inconvenience, hindrance during travel, and consultations in between, which slows referrals, must be handled carefully to reach within the window period.
The most crucial element in stroke care is timely arrival at the center. Kerala is a state that has saturated healthcare facilities. However, the geographical variation and location of stroke centers across the state directly or indirectly affect the travel time or decision-making delay. The pre-hospital delay can be reduced if the stroke center is near the victim. Also, the people's perception of easy accessibility to appropriate healthcare facilities can make their decision-making faster.
Challenges in Establishing Stroke Centers:
Diagnostic facilities and manpower for stroke treatment are more focused than primary care. A CT, ICU care, and Evaluation by a Neurologist are necessary before delivering Golden Hour treatments during stroke. Establishing stroke centers in remote locations and multiple areas is challenging. It is also essential that post-treatment complications, which may require further actions like surgical interventions, are not uncommon. Continuous assessment of stroke patients after thrombolysis by trained healthcare staff is also needed for another 48 hours.
Strategies to Overcome the Challenges:
1) More referral centers: Even though the healthcare facilities lack facilities for stroke diagnosis and care, the trained health experts can mitigate the process by activating nearby stroke centers and fast referral. Sensitizing primary care health workers to recognize stroke symptoms and initiate emergency referrals is crucial.
2) Extensive health education: being a significant reason for mortality and disability, all stakeholders, including healthcare providers, policymakers, and media, need to disseminate health awareness regarding a stroke. stroke symptoms, the need for immediate treatment, and whom to contact must be informed to the community.
3) Strong Emergency Care Network: It is essential to transport the stroke victim to the precise healthcare provider quickly. Also, timely information-sharing coordination saves time and prevents hindrances during healthcare delivery.
References:
1.Kapoor D, Dhiman A, Sharma R, Sundar S. Clinical profile, risk factors and aetiology of young stroke: a tertiary care hospital based study from the Sub-Himalayan region in North India. International Journal of Research in Medical Sciences. 2014;2(4):1355.
2. Iyer R Dr. Prevalence and reasons for pre-hospital delay after acute ischemic stroke: Data from a single tertiary care centre in Coimbatore, South India. Neurology. 2020 Apr 14;94(15).
3.Sharma J, Srivastava P, Bhatia R, Rajan R, Singh R, Goyal V, et al. ‘Prehospital’ delay in acute stroke reperfusion therapy in Delhi: Time for introspection. Journal of the Neurological Sciences. 2019 Oct;405:131–2.
4.Kulkarni G, Mahajan N, Aravinda H. Barriers to Thrombolysis at A Tertiary Care Public Hospital- A Prospective Observational Study from Southern Part of India. Neurology India. 2022;70(3):972.
5.Abraham S, Krishnan Sv, Thaha F, Balakrishnan J, Thomas T, Palatty B. Factors delaying management of acute stroke: An Indian scenario. International Journal of Critical Illness and Injury Science. 2017;7(4):224.
6.Panwar A, Veeramalla M, Valupadas C, Ramesh K, Owais M, Muriki R. Barriers to Stroke Thrombolysis. JOURNAL OF CLINICAL AND DIAGNOSTIC RESEARCH. 2017;
7.Singh S, Kate M, Samuel C, Kamra D, Kaliyaperumal A, Nandi J, et al. Rural Stroke Surveillance and Establishment of Acute Stroke Care Pathway Using Frontline Health Workers in Rural Northwest India: The Ludhiana Experience. Neuroepidemiology. 2021;55(4):297–305.
8.Chhabra M, Gudi SK, Rashid M, Sharma P, Sharma S, Khan H. Assessment of Knowledge on Risk Factors, Warning Signs, and Early Treatment Approaches of Stroke among Community Adults in North India: A Telephone Interview Survey. Journal of Neurosciences in Rural Practice. 2019 Jul;10(03):417–22.
9.Nagendra CV, Kumar TSS, Bohra V, Wilben V, Karan V, Huded V. Factors affecting the effective management of acute stroke: A prospective observational study. Indian Journal of Critical Care Medicine. 2018;22(3):138–43.
10.Vallippalam J, Krishna S, Suresh N, Sunny AA, Karthikeyan, Iyer RS. Stroke education focusing on recognition and response to decrease pre-hospital delay in India: Need of the hour to save hours. Interdisciplinary Neurosurgery. 2021 Dec;26:101309.
11.Revathi S, Kavitha M, Shankar V. Factors associated with prehospital delay in patients with acute stroke in South India. Indian Journal of Community Medicine. 2023;48(1):82.
12.Lyden P, Schwamm LH, Mohl SM. 2022 Update From the American Stroke Association and the Stroke Council. Stroke. 2022 Aug;53(8).
13.Government of India DG of HSM of H and FW. Guidelines for Prevention and Management of Stroke [Internet]. National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases & Stroke (NPCDCS). Government of India; 2019. Available from: https://main.mohfw.gov.in/sites/default/files/Guidelines%20for%20Prevention%20and%20Managment%20of%20Stroke.pdf

Dr. Alaka Chandak
Researcher, Symbiosis International University</p>