Coronary Microvascular Dysfunction in Autoimmune Rheumatic Diseases: Beyond Traditional Markers
.webp)
The article explores coronary microvascular dysfunction (CMD) in autoimmune rheumatic diseases, highlighting increased cardiovascular risks and the diagnostic role of stress cardiac magnetic resonance. Early CMD detection in asymptomatic patients may allow timely intervention, reducing major adverse cardiac events by targeting therapy to manage CMD's impact on cardiovascular health.
Introduction
Autoimmune Rheumatic Diseases (ARDs), such as rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), systemic sclerosis (SS), and antiphospholipid syndrome (APS), involve a heightened risk of cardiovascular diseases (CVDs). One major concern among ARDs patients is coronary microvascular dysfunction (CMD), which contributes to increased cardiovascular morbidity and mortality. Unlike coronary artery disease (CAD), which involves the large coronary arteries, CMD affects the small coronary vessels, posing challenges for diagnosis and treatment.
The Pathophysiology of CMD in ARDs
In ARDs, CMD arises from a combination of endothelial dysfunction, inflammation, oxidative stress, and immune dysregulation. The coronary microcirculation, consisting of small vessels that regulate blood flow to the heart muscle, is highly susceptible to these factors. Functional impairments or structural damage to these small vessels can lead to CMD, characterized by the inability of the coronary microvasculature to appropriately dilate in response to increased myocardial oxygen demands. The dysfunction may be due to reduced nitric oxide (NO) availability, increased reactive oxygen species (ROS) production, and upregulation of pro-inflammatory cytokines like interleukin-17 (IL-17), interferon-gamma (IFN-γ), and tumor necrosis factor-alpha (TNF-α).
Limitations of Coronary Flow Velocity Reserve (CFVR)
Coronary Flow Velocity Reserve (CFVR), assessed through echocardiography, has been a traditional method for diagnosing CMD. It evaluates the capacity of coronary blood flow to increase during stress compared to its baseline state. While CFVR is a reliable indicator for CMD in ARDs patients, its effectiveness can be limited due to the complex mechanisms involved in these diseases. CFVR is less sensitive in detecting microvascular impairments that do not lead to significant flow changes, particularly in cases where CMD results from microvascular inflammation or vasospasm rather than stenosis.
Advancements in Diagnostic Imaging: Stress Cardiac Magnetic Resonance (CMR)
Stress Cardiac Magnetic Resonance (CMR) has emerged as a superior, non-invasive diagnostic tool for assessing CMD in ARDs. Unlike CFVR, which may not detect all forms of microvascular dysfunction, stress CMR provides a comprehensive evaluation of myocardial perfusion, ischemia, and viability. Using pharmacologic agents such as adenosine or regadenoson, stress CMR induces hyperemia and captures detailed images of myocardial blood flow. The Myocardial Perfusion Reserve Index (MPRI), a semiquantitative measure derived from stress CMR, serves as a robust marker of coronary microvascular health. (Figure)
Clinical Evidence of Stress CMR in ARDs Patients
Recent studies have demonstrated the utility of stress CMR in identifying CMD among patients with ARDs. For instance, women with SLE exhibited significantly reduced MPRI values compared to healthy controls, underscoring impaired coronary microvascular function in the absence of significant coronary artery stenosis. In systemic sclerosis (SS) patients, stress CMR has revealed non-segmental myocardial fibrosis and hypoperfusion, which correlate with reduced MPRI and heightened cardiovascular risk. These findings highlight the potential of stress CMR to identify CMD even in asymptomatic patients, enabling early intervention and targeted treatment.
Pathogenic Mechanisms of CMD in ARDs
The pathogenesis of CMD in ARDs is multifactorial and remains a subject of investigation. Endothelial dysfunction plays a pivotal role in CMD, driven by the imbalance between vasodilatory and vasoconstrictive factors. Oxidative stress, a key factor in ARDs, contributes to endothelial dysfunction by reducing NO bioavailability and increasing ROS production. Inflammatory cytokines, such as TNF-α, IL-6, and IL-17, activate NADPH oxidases (NOX), further promoting ROS generation. This inflammatory milieu not only affects endothelial function but also contributes to vascular remodeling and arteriolar rarefaction, exacerbating CMD. Additionally, immune cells such as T-cells, natural killer (NK) cells, and monocytes play a role in endothelial dysfunction in ARDs. These cells release cytokines and pro-inflammatory mediators that trigger microvascular inflammation and vasoconstriction. For example, NK cells can induce arteriolar vasoconstriction, while CD28 null T-cells produce TNF-α and IFN-γ, leading to oxidative stress and CMD.
Prognostic Implications of CMD in ARDs
CMD is increasingly recognized as a significant predictor of adverse cardiovascular outcomes in ARDs patients. A reduced MPRI in stress CMR correlates with an elevated risk of major adverse cardiovascular events (MACEs), such as myocardial infarction, stroke, and heart failure. Identifying CMD early in ARDs patients, even before overt clinical symptoms arise, is critical for preventing these complications and improving long-term outcomes.
Therapeutic Approaches to CMD in ARDs
The management of CMD in ARDs involves both pharmacologic and non-pharmacologic strategies. Current treatments focus on improving endothelial function, reducing inflammation, and managing risk factors associated with CMD. Treatments including beta-blockers, calcium channel blockers, and nitrates have proven effective in alleviating angina symptoms and enhancing exercise tolerance in patients with CMD. Angiotensin-converting enzyme inhibitors (ACEIs), angiotensin II receptor blockers (ARBs), and statins are also beneficial, given their roles in modulating endothelial function, reducing oxidative stress, and exerting anti-inflammatory effects. In addition, non-pharmacologic interventions, such as lifestyle modifications including smoking cessation, weight management, and regular physical activity, are essential for mitigating cardiovascular risk in CMD patients. These interventions have been shown to enhance coronary flow reserve and alleviate symptoms of CMD.
Future Directions in CMD Research and Management
While stress CMR has provided significant advancements in the detection and management of CMD in ARDs, further research is needed to refine its diagnostic and prognostic capabilities. Large-scale, multicenter studies are essential to validate the role of MPRI in predicting MACEs across diverse patient populations and to establish standardized protocols for CMD assessment in clinical practice. Moreover, the development of targeted therapies aimed specifically at CMD in ARDs could revolutionize treatment approaches. Potential therapies might focus on modulating immune responses, reducing oxidative stress, or directly targeting endothelial function. For example, biological agents that inhibit TNF-α or IL-6 could offer dual benefits by managing ARDs symptoms while improving CMD outcomes.
Conclusion
Coronary microvascular dysfunction is a significant but frequently overlooked factor in cardiovascular morbidity and mortality among patients with autoimmune rheumatic diseases. Beyond traditional diagnostic measures like CFVR, advanced imaging techniques such as stress CMR provide a comprehensive evaluation of CMD, enabling early detection and intervention. As our understanding of CMD in ARDs evolves, integrating these diagnostic tools into routine clinical practice could significantly improve patient outcomes and reduce cardiovascular complications in this high-risk population.
Figure legend
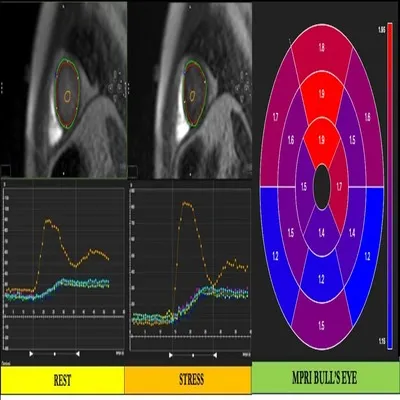
This figure illustrates myocardial perfusion imaging using magnetic resonance imaging (MRI) at rest and during stress, accompanied by a bull's eye map showing the Myocardial Perfusion Reserve Index (MPRI).
1. Left Panel (REST):
- The left MRI image shows the cross-sectional view of the heart during rest. The red and green contours outline the endocardium and epicardium, respectively. The yellow contour highlights the region of interest for perfusion analysis.
- Below the image is a graph plotting signal intensity (SI) against time (seconds), indicating myocardial perfusion during the resting state. The yellow curve represents the time-intensity curve, showing the peak and washout phases of contrast agent uptake.
2. Middle Panel (STRESS):
- The middle MRI image shows the cross-sectional view of the heart during stress. Similar contours (red, green, and yellow) are used to define anatomical boundaries and regions of interest.
- The corresponding graph below displays signal intensity changes over time during stress. The curve reflects increased myocardial blood flow during stress conditions compared to rest, which helps in assessing myocardial perfusion reserve.
3. Right Panel (MPRI Bull's Eye Map):
- The right panel shows a polar bull's eye map representing the Myocardial Perfusion Reserve Index (MPRI) across different myocardial segments. Each segment is color-coded according to the MPRI values, with red indicating higher values and blue indicating lower values.
- The MPRI is a ratio of stress perfusion to rest perfusion and is used to identify areas with potential perfusion defects or microvascular dysfunction. Higher MPRI values suggest better myocardial perfusion, while lower values may indicate areas of reduced blood flow or ischemia.
Color Bar (Right Side):
- The color bar provides a scale for interpreting the MPRI values on the bull's eye map, ranging from 1.15 (blue) to 1.95 (red).
.webp)








