Beyond Efficiency: Rethinking Workforce Optimisation in Healthcare

Why burnout, moral injury, and unsustainable work cultures are silently eroding performance—and how people-centric leadership can restore resilience, productivity, and care quality
Workforce optimisation in healthcare cannot rely on efficiency metrics alone. This article examines how burnout, moral injury, and unsustainable work cultures undermine productivity, retention, and care quality. It proposes people-centric, leadership-driven strategies that integrate wellbeing, social sustainability, and operational design to build resilient, high-performing healthcare workforces.
Introduction:
Workforce optimisation has become one of the most frequently invoked phrases in contemporary healthcare leadership discourse. Across Asia, hospital systems are expanding rapidly, patient volumes are rising, and operational pressures are intensifying. In response, optimisation has largely been interpreted as doing more with less, shorter turnaround times, tighter staffing ratios, higher bed occupancy, and relentless performance monitoring. While these measures may temporarily improve efficiency indicators, they have also produced a quieter, more dangerous consequence: the gradual depletion of the healthcare workforce itself.
Healthcare systems have optimised processes while underestimating the cost borne by the people who deliver care. The result is a paradox increasingly visible across Asian hospitals: productivity targets are met on paper even as burnout, disengagement, attrition, and compromised care quality rise beneath the surface. Workforce optimisation, when divorced from human sustainability, becomes self-defeating. The system appears efficient until the workforce begins to fracture. This tension is particularly acute in Asia, where healthcare delivery operates at the intersection of high patient demand, workforce shortages, hierarchical organisational cultures, and deep-rooted stigma surrounding mental health. To rethink workforce optimisation meaningfully, healthcare leaders must confront the data they have long sidestepped—and reframe wellbeing not as a soft issue, but as a strategic imperative.
The Data Healthcare Can No Longer Ignore
Burnout among healthcare professionals is no longer anecdotal or confined to Western systems. Large-scale studies across Asia consistently demonstrate high levels of emotional exhaustion, depersonalization, and reduced professional efficacy among doctors and nurses. The World Health Organisation has repeatedly warned that global health systems are facing a workforce crisis, estimating a projected shortfall of 10 million healthcare workers worldwide by 2030, with significant impact in low- and middle-income regions, including large parts of Asia [1].
In India, multicenter studies conducted in tertiary hospitals have reported burnout prevalence among physicians ranging from 44% to over 60%, particularly in high-intensity specialities and outpatient departments with extreme patient volumes [2]. Similar patterns are seen across Southeast Asia. A national survey in Singapore found that nearly half of physicians reported symptoms consistent with burnout, despite the country’s highly developed healthcare infrastructure [3]. In Gulf Cooperation Council (GCC) countries, where healthcare systems rely heavily on expatriate clinicians, studies have shown burnout rates exceeding 50%, compounded by job insecurity, long working hours, and limited organisational support [4].
Burnout is not merely an emotional state; it carries measurable organisational consequences. The OECD has demonstrated a clear association between poor worker wellbeing and reduced productivity, increased absenteeism, and higher turnover costs across service industries, including healthcare [5]. Replacing a single physician can cost hospitals between one and two times the clinician’s annual salary when recruitment, onboarding, and lost productivity are accounted for [6]. Yet these costs rarely appear in optimisation dashboards.
Table 1. Selected Evidence on Burnout and Workforce Impact in Asian Healthcare
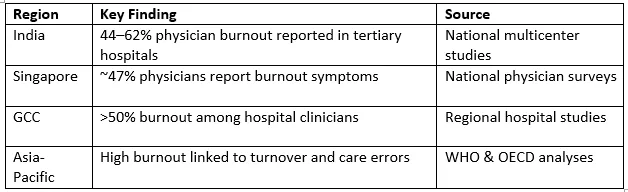
These figures are not signals of individual fragility. They are indicators of systems operating beyond sustainable human limits.
Burnout versus Moral Injury: A Critical Distinction
Burnout is often framed as a personal resilience problem—a failure to cope. Moral injury, however, exposes the deeper ethical fracture within healthcare systems. Moral injury occurs when clinicians are repeatedly placed in situations where institutional constraints prevent them from providing the care they know is right. Chronic understaffing, unrealistic patient loads, administrative pressures, and productivity-driven decision-making force clinicians into ethical compromises that erode professional identity and meaning.
Unlike burnout, moral injury does not improve with yoga sessions or resilience workshops. It manifests as disengagement, cynicism, and ultimately withdrawal from the profession. Asian healthcare systems, with their strong hierarchies and limited channels for upward feedback, may unintentionally intensify moral injury by silencing clinician concerns. When healthcare workers feel unheard, unsupported, and ethically compromised, optimisation efforts lose legitimacy.
This distinction matters for leadership. Addressing burnout without addressing moral injury is akin to treating symptoms while ignoring the disease. Workforce optimisation strategies that fail to acknowledge ethical distress will continue to struggle with retention, trust, and performance.
Why Asian Healthcare Is Uniquely Vulnerable
Asian healthcare systems face structural pressures that make unsustainable optimisation particularly dangerous. Rapid urbanisation, ageing populations, and epidemiological transitions have dramatically increased demand for healthcare services. In many countries, outpatient clinics routinely see volumes that far exceed international norms. Clinicians are expected to move faster, document more, and deliver consistently high patient satisfaction—often with limited decision-making autonomy.
Cultural factors further complicate the picture. Hierarchical organisational structures discourage open dialogue about workload, fatigue, and psychological distress. Mental health stigma persists not only among patients but within the healthcare workforce itself. Admitting struggle is frequently equated with weakness, particularly among senior clinicians and leaders.
In private healthcare systems across Asia, aggressive growth models and competitive pressures reinforce a narrow definition of productivity. Key performance indicators focus on patient throughput, revenue generation, and utilization metrics, while human sustainability indicators remain peripheral. This imbalance creates a false economy: short-term efficiency gains are achieved at the cost of long-term workforce stability.
Rethinking Workforce Optimisation: From Extraction to Sustainability
True workforce optimisation must shift from extraction-based models to sustainability-based design. This requires reframing healthcare workers not as endlessly scalable resources, but as skilled professionals whose cognitive, emotional, and ethical capacities have limits.
Leadership accountability sits at the center of this shift. When leaders acknowledge that burnout and moral injury are system-generated, responsibility moves from individuals to organisations. Sustainable workload design becomes a strategic priority, not a concession. Evidence from high-performing healthcare organisations shows that reasonable patient-to-clinician ratios, protected rest periods, and autonomy in clinical decision-making are associated with better patient outcomes and higher staff retention [7].
Psychological safety is equally critical. The ability to speak openly about errors, fatigue, and ethical concerns without fear of reprisal is strongly linked to team performance and patient safety. Asian hospitals that have invested in confidential support systems, peer-support programs, and leadership training in empathetic management report measurable improvements in engagement and reduced turnover [8].
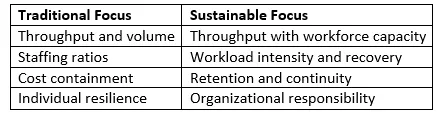
Importantly, optimization metrics must evolve. Measuring output without measuring human cost distorts decision-making. Progressive systems now integrate indicators such as staff engagement, burnout prevalence, absenteeism, and retention alongside traditional productivity measures. This integration does not weaken performance; it strengthens it.
Table 2. Traditional vs Sustainable Workforce Optimization
What Healthcare Leaders Can Do Now
The path forward does not require radical disruption, but deliberate recalibration. Leaders must first acknowledge that current optimisation models carry hidden costs. Openly recognising burnout and moral injury as system outcomes signals psychological safety and restores trust. Leadership development programmes should priorities human-centered management, equipping leaders to recognise distress, manage workloads ethically, and align operational decisions with workforce wellbeing.

At the organisational level, workforce planning must become anticipatory rather than reactive. Data on absenteeism, turnover intent, and engagement should inform staffing models before crises emerge. Normalising conversations about mental health within healthcare teams reduces stigma and encourages early intervention.
For hospital boards and policymakers, the message is clear: sustainable workforce optimisation is inseparable from care quality, financial resilience, and public trust. Systems that protect their workforce protect their future.
Conclusion: Optimisation That Sustains
Healthcare cannot optimise its way out of a workforce crisis by demanding more from already depleted professionals. Efficiency achieved through exhaustion is not efficiency at all—it is deferred failure. Asian healthcare systems stand at a critical inflection point. By reimagining workforce optimisation through the lens of social sustainability, leadership accountability, and ethical care delivery, healthcare organisations can build systems that perform not only today but also endure tomorrow.
Workforce optimisation must stop asking how much more can be extracted and start asking how long the system is meant to last.
Numbered References
- World Health Organization. Global Strategy on Human Resources for Health: Workforce 2030. WHO; 2016.
- Kumar S, et al. Burnout among physicians in tertiary care hospitals in India. Indian J Med Ethics. 2020.
- Lee PT, et al. Physician burnout in Singapore: A national survey. Ann Acad Med Singapore. 2019.
- Al-Jabri B, et al. Burnout among healthcare professionals in GCC countries. BMJ Open. 2021.
- OECD. Mental Health and Work: Performance and Well-Being. OECD Publishing; 2014.
- Han S, et al. Estimating the cost of physician turnover. Am J Med Qual. 2019.
- Shanafelt TD, et al. Impact of organisational leadership on physician wellbeing. Mayo Clin Proc. 2015.
- West CP, et al. Interventions to prevent and reduce physician burnout. Lancet. 2018.









