Venous Thromboembolism Prophylaxis in Patients with Acute Ischemic Stroke
.webp)
Venous thromboembolism (VTE), was first described in Ancient India around 600BC. Stroke patients face a higher VTE prevalence. VTE prophylaxis using low molecular weight heparin (LMWH) is standard, except in acute ischaemic stroke where it remains debated. Comparing LMWH and unfractionated heparin (UFH) for VTE prevention in stroke patients, we found no statistically significant difference between the two, although LMWH showed favourable results. LMWH also demonstrated superiority in preventing symptomatic DVT. Surprisingly, LMWH was safer, with no intracranial hemorrhage complications, unlike UFH. Future research should focus on the novel oral anticoagulants which hold promise.
When was VTE first described?
The earliest description of Venous thromboembolism (VTE), which includes conditions like deep vein thrombosis (DVT) and pulmonary embolism (PE), come from Ancient India around 600 to 900 BC. However, the understanding of its causes and mechanisms was limited during this time. It was not until western researchers, starting between 17th to 19th centuries, that significant progress in comprehending VTE was made1 . They delved into the anatomy, physiology, and pathology of both DVT and PE. Notably, this period saw advancements beyond traditional practises like vessel ligation and immobilisation, eventually leading to the emergence of anticoagulation therapy as the standard of care2.
The Virchow’s triad, first described by Rudolf Virchow in 1856, played a significant role in the understanding of the pathology and pathogenesis of VTE3. Broken down into its components, it consists of hypercoagulability, haemodynamic stasis, and endothelial injury. Various risk factors contribute to hypercoagulability, like genetic mutations (factor V Leiden and prothrombin), deficiencies in antithrombin III, protein C, or protein S, nephrotic syndrome, malignancy, among others. Stasis occurs as blood flow slows down or becomes stagnant. Extended immobility, long surgical operations, or varicose veins are common causes of venous stasis. Finally, damage to the endothelial lining of blood vessels due to vessel piercings, shear stress, hypertension, or contact with procoagulant surfaces (such as bacteria, foreign materials, or activated platelets) completes the triad.
Stroke patients are at higher risk
Most patients presenting with a VTE typically exhibit only one of the components of Virchow’s triad. However, patients with acute ischaemic stroke face a significantly higher risk of VTE compared to other patients because they often have two components of the triad. On one hand, hemiplegia or limb paralysis limits mobility in stroke patients. On the other hand, stroke patients are in a hypercoagulable state. This dual influence contributes to the higher prevalence of VTE in hospitalised stroke patients, reaching up to 75%4 compared to 5-10% in other patient populations5.
The majority of these VTEs are DVTs6, and their clinical significance varies according to the thrombus location (proximal vs. distal) and the presence or absence of any accompanying symptoms7. Up to half the DVTs will lead to PE8. Although the majority of PEs are a complication of symptomatic rather than asymptomatic DVTs, their clinical significance is the same9. Only 1-3% of critically ill patients will experience a PE, but PEs account for about half of early deaths in stroke patients10.
The optimal agent for VTE prophylaxis
VTE prophylaxis using low molecular weight heparin (LMWH) has indeed become the standard of care for many patient populations. Except for obese patients and those with kidney failure, LMWH is considered more effective than unfractionated heparin (UFH), safer, and easier to administer11. The convenience of once-daily dosing with LMWH has contributed to its widespread adoption in clinical practise. VTE prophylaxis in patients with acute ischaemic stroke, however, has been a topic of debate. Guidelines published by the American Stroke Association do not specify the optimal agent for prophylaxis, stating that there is uncertainty regarding any benefit of prophylactic-dose LMWH over prophylactic-dose UFH12.
As a result, many neurointensivists have been reluctant to use LMWH for VTE chemoprophylaxis. Enoxaparin, the most famous LMWH, was traditionally believed to increase the risk of hemorrhagic conversion of ischaemic strokes when compared to UHF13. However, newer studies are refuting this old belief10,14,15. These complications, coupled with the shorter half-life of UFH and the presence of an effective reversal agent, protamine sulfate, are also hindering LWMH adoption.
Our research
What are the advantages of LMWH over UHF for VTE prevention in stroke patients? Is one of these anticoagulants superior? And is UFH truly safer than LMWH in terms of hemorrhagic conversion? To address these questions, among others, we conducted a large-scale, single-centre retrospective cohort study16.
After screening 909 patients admitted to the NeuroICU with the diagnosis of acute ischaemic stroke, 275 patients were excluded, leaving 643 patients who were enrolled in the study and were divided according to the VTE chemoprophylactic agent they received: LMWH (170 patients) or UFH (464 patients). The collected baseline patient characteristics included age, sex, weight, length of hospitalisation, and prophylactic duration, among others. The primary outcome was the incidence of VTE, which was further classified into DVT and PE. Specifically, DVTs were subclassified into proximal vs. distal and symptomatic vs. asymptomatic. PEs were subclassified into massive vs. segmental vs. subsegmental, as well as symptomatic vs. asymptomatic. Additionally, the incidence of intracranial hemorrhage was also recorded in both groups.
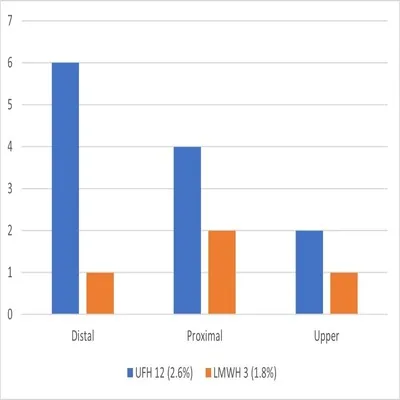
The results were somewhat surprising. There was no statistically significant difference between both anticoagulants in terms of VTE prevention, although the numbers favoured LMWH over UFH (1.8% vs. 4.1%). Regarding PE, there were 9 cases in the UFH group compared to none in the LMWH, but these numbers did not reach statistical significance. Additionally, there were 12 DVTs in the UFH group and 3 in the LMWH group, but the difference was not statistically significant (Figure 1). One could argue that with a larger sample size, the difference would likely become statistically significant. The low number of events might have also contributed to the absence of statistical difference. All DVTs in the UFH group were symptomatic compared to only one symptomatic DVT in the LMWH group. This difference was statistically significant and further proves the superiority of LMWH affecting, both quality and quantity of VTEs. Even more surprising, however, were the rates of intracranial hemorrhage. Eighteen patients receiving UFH experienced hemorrhagic conversion during their hospital stay, while none of the patients receiving LMWH had this complication.
Conclusions and future directions
So, what does this mean? LMWH appears to be as effective as UFH heparin for VTE prevention, but it is safer. This could be explained by the fact that LMWH has more antithrombic activity than anticoagulant activity when compared to UFH. Neurointensivists should be encouraged to use LMWH for VTE prevention.
Future research on VTE prevention and treatment in patients with stroke is crucial for improving patient outcomes. This research should focus on several key areas. First, developing quantitative risk assessment tools for VTE and bleeding in critically ill patients can help identify those at high risk and guide personalised prevention strategies. Second, enhancing prophylactic medication use is essential to reduce healthcare-associated VTE in high-risk patients. Investigating barriers to adherence will contribute to better outcomes.
Finally, stroke-specific research should also concentrate on hemorrhagic stroke patients. Similar to stroke patients, VTE is a significant concern in patients with intracerebral hemorrhage (ICH). Controversy still exists about chemoprophylaxis and the use of anticoagulants due to risk for recurrent ICH. Future studies should explore optimal anticoagulants, timing of initiation, and dosing. Although initiating chemoprophylaxis with UFH or LMWH within 24–48 hours of ICH onset appears safe, novel oral anticoagulants (NOACs) hold promise for VTE prevention and treatment and should be further studied.
References:
- Goodman LR. In search of venous thromboembolism: the first 2913 years. AJR Am J Roentgenol. Oct 2013;201(4):W576-81. doi:10.2214/AJR.13.10604
- Hurt J, Maday K, Michelle Brown, Harrelson P. Deep Vein Thrombosis: History and Evolution of Treatment. https://www.clinicaladvisor.com/home/features/deep-vein-thrombosis-history-and-evolution-of-treatment/
- Kumar DR, Hanlin E, Glurich I, Mazza JJ, Yale SH. Virchow's contribution to the understanding of thrombosis and cellular biology. Clin Med Res. Dec 2010;8(3-4):168-72. doi:10.3121/cmr.2009.866
- Khan MT, Ikram A, Saeed O, et al. Deep Vein Thrombosis in Acute Stroke - A Systemic Review of the Literature. Cureus. Dec 23 2017;9(12):e1982. doi:10.7759/cureus.1982
- Gao X, Zeng L, Wang H, et al. Prevalence of Venous Thromboembolism in Intensive Care Units: A Meta-Analysis. Journal of Clinical Medicine. Nov 11 2022;11(22):6691. doi:10.3390/jcm11226691
- Kelly J, Rudd A, Lewis R, Hunt BJ. Venous thromboembolism after acute stroke. Stroke. Jan 2001;32(1):262-7. doi:10.1161/01.str.32.1.262
- Kabashneh S, Singh V, Alkassis S. A Comprehensive Literature Review on the Management of Distal Deep Vein Thrombosis. Cureus. May 10 2020;12(5):e8048. doi:10.7759/cureus.8048
- Hirsh J, Hoak J. Management of deep vein thrombosis and pulmonary embolism. A statement for healthcare professionals. Council on Thrombosis (in consultation with the Council on Cardiovascular Radiology), American Heart Association. Circulation. Jun 15 1996;93(12):2212-45. doi:10.1161/01.cir.93.12.2212
- Hirmerova J, Seidlerova J, Chudacek Z. The Prevalence of Concomitant Deep Vein Thrombosis, Symptomatic or Asymptomatic, Proximal or Distal, in Patients With Symptomatic Pulmonary Embolism. Clin Appl Thromb Hemost. Nov 2018;24(8):1352-1357. doi:10.1177/1076029618779143
- Kamphuisen PW, Agnelli G. What is the optimal pharmacological prophylaxis for the prevention of deep-vein thrombosis and pulmonary embolism in patients with acute ischemic stroke? Thromb Res. 2007;119(3):265-74. doi:10.1016/j.thromres.2006.03.010
- Schunemann HJ, Cushman M, Burnett AE, et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: prophylaxis for hospitalized and nonhospitalized medical patients. Blood Adv. Nov 27 2018;2(22):3198-3225. doi:10.1182/bloodadvances.2018022954
- Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. Dec 2019;50(12):e344-e418. doi:10.1161/STR.0000000000000211
- Dennis M, Caso V, Kappelle LJ, Pavlovic A, Sandercock P, European Stroke O. European Stroke Organisation (ESO) guidelines for prophylaxis for venous thromboembolism in immobile patients with acute ischaemic stroke. Eur Stroke J. Mar 2016;1(1):6-19. doi:10.1177/2396987316628384
- Sherman DG, Albers GW, Bladin C, et al. The efficacy and safety of enoxaparin versus unfractionated heparin for the prevention of venous thromboembolism after acute ischaemic stroke (PREVAIL Study): an open-label randomised comparison. Lancet. Apr 21 2007;369(9570):1347-1355. doi:10.1016/S0140-6736(07)60633-3
- Shorr AF, Jackson WL, Sherner JH, Moores LK. Differences between low-molecular-weight and unfractionated heparin for venous thromboembolism prevention following ischemic stroke: a metaanalysis. Chest. Jan 2008;133(1):149-55. doi:10.1378/chest.07-1826
- Al Turk M, Abraham M. Incidence of Symptomatic Venous Thromboembolisms in Stroke Patients. J Intensive Care Med. Mar 26 2024;doi:10.1177/08850666241242683
.webp)








