Automated FFR Assessment
Artificial intelligence in the catheterisation laboratory

Physiologic assessment of coronary lesion significance is underused in common practice. Recently an artificial intelligence-based algorithm was developed to derive fractional flow reserve from angiographic images with an accuracy level of 90 per cent leading to its approval for distribution in Europe and the launch of a pivotal trial for FDA clearance.
Coronary physiological assessment has become the gold standard for myocardial ischemia testing1, 2. It has been shown to improve outcome and reduce revascularisation in patients with chronic coronary artery disease 3, 4, along with guiding complete revascularisation and reduction in the combined outcome of death or myocardial infarction in patients with acute coronary syndrome5. The results of a coronary physiological assessment have been shown to change the treatment strategy in more than 40 per cent of cases and save inappropriate stents and bypass surgeries6. Indeed, the burden of inappropriate revascularisation has been reported to be in excess of 30 per cent, reaching a cost of US$4 billion. Moreover, a recent trial showed that in 24 per cent of cases the physiologic assessment was still pathologic following treatment of the coronary lesion, mainly due to focal residual stenosis7.
Nonetheless, despite its proven benefit for the patients, physiological assessment is performed in less than 10 per cent of interventions8, due to several limitations that include the time required for the set-up of the system, its price, patients comfort and safety especially when performing an invasive assessment and administering adenosine for fractional flow reserve (FFR) test.
In order to address these issues, several angiography-based softwares have been developed using 3-dimensional coronary flow dynamics simulation. These software solutions require certain views and annotation of the vessel in question, thereby interrupting the workflow of the procedure in order to perform the test. The analysis requires between 5 and 15 minutes for each vessel and has a learning curve.
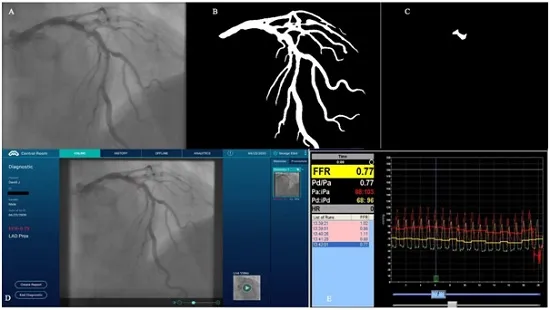
Artificial intelligence (AI)-based software such as developed by Medhub (Tel Aviv, Israel), using machine learning and deep learning algorithms that analyse the images taken by the operator and provides an automated FFR assessment without the need for views adjustment or vessel annotation (AutocathFFR). The software is able to track each lesion prior and post treatment in order to provide a post procedural FFR value for further risk assessment for future adverse events with the vision of helping physicians to reach an accurate diagnosis and provide better care for coronary heart disease patients (Figure). The automated nature of AutocathFFR integrates seamlessly into the catheterisation workflow without any manual requirements from the operator or stuff. It allows rapid detection and evaluation coronary stenosis on the entire coronary tree thereby, helps the operators to identify significant lesions that might be otherwise missed. This technology was presented in leading cardiology conferences including Innovation in Cardiovascular Interventions in Tel-Aviv, Israel and Cardiovascular Research Technologies in Washington DC, USA.
Recently MedHub completed its feasibility study for CE mark and the Israeli Ministry of Health regulatory authority comparing its AutoCath FFR estimation based on AI and angiography images to pressure-wire based FFR in 31 patients9. The goal was reaching over 70 per cent sensitivity and 75 per cent specificity, similar to prior trials of angiography based FFR based on computational fluid dynamics simulations. Indeed, the trial results showed a sensitivity, specificity, positive and negative predictive value of 88per cent, 93per cent, 94per cent and 87per cent respectively, reaching an accuracy level of 90per cent in detecting FFR above or below 0.8. Moreover, the software detected 96per cent of coronary lesions with FFR > 0.9 and 100per cent of coronary lesions. These results are encouraging and provided the base for approval for use in Europe and Israel.
The nature of the algorithm and its utilisation of deep learning methods offer additional significant advantage. On top of its automated rapid FFR assessment and automated stenosis detection capability, the software allows users to analyse and extract information from previous procedures and analyse them retrospectively. The algorithm itself is able to self-learn and improve and subsequently be updated from time to time due to continuous learning. Therefore, further improvements in precision and accuracy are expected as the company works vigorously to further improve the algorithm and finetune its output.
An upcoming multicenter trial is expected for FDA approval with centers in Israel and Europe comparing the algorithm results with pressure wire based FFR, in addition to a 510K application for an FDA clearance with the intention to distribute the software in the USA.
This technology has the potential to display FFR values almost in real time, parallel to the acquisition of the diagnostic images. This may potentially improve the quality in which we make clinical decisions in the catheterisation laboratory, as well as save resources.
Acknowledgement
We would like to thank and acknowledge the contribution of Igal Loevsky in the development, Dr. Yair Feld and Prof Ariel Roguin for their contribution during the development and trial process.
References
1. De Bruyne B, Pijls NH, Kalesan B, Barbato E, Tonino PA, Piroth Z, Jagic N, Mobius-Winkler S, Rioufol G, Witt N, Kala P, MacCarthy P, Engstrom T, Oldroyd KG, Mavromatis K, Manoharan G, Verlee P, Frobert O, Curzen N, Johnson JB, Juni P, Fearon WF and Investigators FT. Fractional flow reserve-guided PCI versus medical therapy in stable coronary disease. The New England journal of medicine. 2012;367:991-1001.
2. Pijls NH, De Bruyne B, Peels K, Van Der Voort PH, Bonnier HJ, Bartunek JKJJ and Koolen JJ. Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. The New England journal of medicine. 1996;334:1703-8.
3. van Nunen LX, Zimmermann FM, Tonino PA, Barbato E, Baumbach A, Engstrom T, Klauss V, MacCarthy PA, Manoharan G, Oldroyd KG, Ver Lee PN, Van't Veer M, Fearon WF, De Bruyne B, Pijls NH and Investigators FS. Fractional flow reserve versus angiography for guidance of PCI in patients with multivessel coronary artery disease (FAME): 5-year follow-up of a randomised controlled trial. Lancet. 2015;386:1853-60.
4. Xaplanteris P, Fournier S, Pijls NHJ, Fearon WF, Barbato E, Tonino PAL, Engstrom T, Kaab S, Dambrink JH, Rioufol G, Toth GG, Piroth Z, Witt N, Frobert O, Kala P, Linke A, Jagic N, Mates M, Mavromatis K, Samady H, Irimpen A, Oldroyd K, Campo G, Rothenbuhler M, Juni P, De Bruyne B and Investigators F. Five-Year Outcomes with PCI Guided by Fractional Flow Reserve. The New England journal of medicine. 2018;379:250-259.
5. Smits PC, Abdel-Wahab M, Neumann FJ, Boxma-de Klerk BM, Lunde K, Schotborgh CE, Piroth Z, Horak D, Wlodarczak A, Ong PJ, Hambrecht R, Angeras O, Richardt G, Omerovic E and Compare-Acute I. Fractional Flow Reserve-Guided Multivessel Angioplasty in Myocardial Infarction. The New England journal of medicine. 2017;376:1234-1244.
6. Van Belle E, Rioufol G, Pouillot C, Cuisset T, Bougrini K, Teiger E, Champagne S, Belle L, Barreau D, Hanssen M, Besnard C, Dauphin R, Dallongeville J, El Hahi Y, Sideris G, Bretelle C, Lhoest N, Barnay P, Leborgne L, Dupouy P and Investigators of the Registre Francais de la F-RF. Outcome impact of coronary revascularisation strategy reclassification with fractional flow reserve at time of diagnostic angiography: insights from a large French multicenter fractional flow reserve registry. Circulation. 2014;129:173-85.
7. Jeremias A, Davies JE, Maehara A, Matsumura M, Schneider J, Tang K, Talwar S, Marques K, Shammas NW, Gruberg L, Seto A, Samady H, Sharp A, Ali ZA, Mintz G, Patel M and Stone GW. Blinded Physiological Assessment of Residual Ischemia After Successful Angiographic Percutaneous Coronary Intervention: The DEFINE PCI Study. JACC Cardiovascular interventions. 2019;12:1991-2001.
8. Harle T, Zeymer U, Hochadel M, Zahn R, Kerber S, Zrenner B, Schachinger V, Lauer B, Runde T and Elsasser A. Real-world use of fractional flow reserve in Germany: results of the prospective ALKK coronary angiography and PCI registry. Clinical research in cardiology : official journal of the German Cardiac Society. 2017;106:140-150.
9. Roguin A, Dogosh A, Feld Y, Konigstein M, Lerman A and Koifman E. Early Feasibility of Automated Artificial Intelligence Angiography Based Fractional Flow Reserve Estimation. The American journal of cardiology. 2020.
Figure Legend
Case example of a proximal LAD lesion (panel A), AutocathFFR automatic vessel segmentation (panel B) and stenosis detection (panel C) and FFR derivation of 0.75 (panel D), while wire based FFR assessment was 0.77 (panel E).







-(1).webp)
