Strategies for Early Detection of Lung Cancer
Reducing mortality in Taiwan

Lung cancer is leading cancer death in Taiwan for several years. Past studies have found that chest radiography or sputum screening does not effectively reduce lung cancer mortality. Kaohsiung Veterans General Hospital-led team developed modified Lung-RADS system for prolong implementation of lung cancer screening program in Asian population with high prevalence of non-smoking related lung cancer(H-T Hsu, et al.,2018).Their long-term study found that more early stage lung cancer detected and lung cancer mortality continued to decline after gradual implementation of lung cancer screening program(FZ Wu, et al.,2020).
Introduction
Lung cancer is still a worldwide leading cause of cancer death, even in this era of low-dose CT for lung cancer screening. Lung cancer mortality rate is the highest among the top ten cancers in Taiwan. There is an increasing trend in non-smoking related lung cancer in Taiwan, especially in middle-age women(FZ Wu, et al.,2016). However, the mechanism for its rise has not been adequately clarified. Since the majority of death occurs at advanced stages of lung cancer, prevention strategy is important. About 70 per cent of lung cancer patients are diagnosed at late stage in Taiwan, and treating them at early stage can save their lives. The Kaohsiung Veterans General Hospital Cardiothoracic Imaging Center has a comprehensive lung cancer screening program. The team recently reported that lung cancer screening could be performed efficiently and effectively in South Taiwan for preventing people death from lung cancer.”We established a multidisciplinary Lung Cancer Screening Program (from diagnosis to treatment) consisting of specialists in chest radiology, thoracic surgery, pulmonary medicine, and lung pathology,” says Dr. Fu-Zong,Wu.
The clinical characteristics difference between screened and non-screened lung cancer
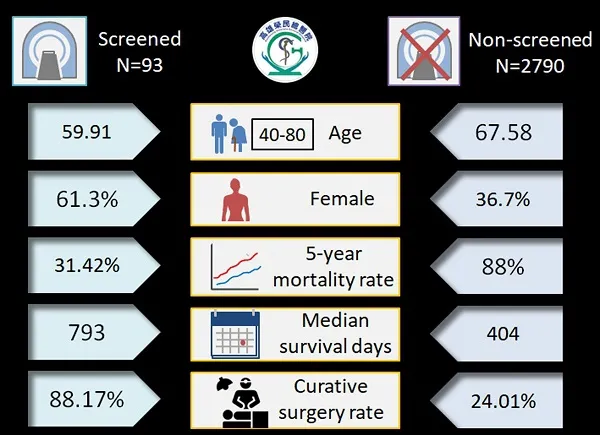
Under the leadership of Dr. Wu, the medical team of Kaohsiung Veterans General Hospital was the first in Taiwan to prove prolong large-volume implementation with low-dose lung computed tomography (CT) and thus gradually lung cancer mortality decreased. In addition, Dr. Wu also applies modified lung imaging reporting and data system (Lung-RADS) for low-dose computed tomography (LDCT) structure report(H-T Hsu, et al.,2018). A structural reporting system could improve diagnostic accuracy and reduce false positive rates. This classification uses a double threshold to distinguish between aggressive or indolent lung cancers to reduce the issue of overdiagnosis issues which almost likely to occur during lung cancer screening process(PA Chen, et al.,2018, FZ Wu, et al.,2017, EK Tang, et al.,2019). Research team also uses big data to link medical imaging database with lung cancer registration database. According to the study report, the screening group was younger and had a higher proportion of women when diagnosed with lung cancer(FZ Wu, et al.,2019). In addition, the study results also demonstrated the screened group showed significantly better surgical and survival outcomes than the non-screened group in Asian populations with the high prevalence of non–smoking-related lung cancer (age between 40-80 year-old) shown in Figure 1.
LDCT screening for lung cancer give rise to a beneficial stage shift with improving survival rate in Asian population
Dr. Fu-Zong, Wu is the lead imaging investigator at cardiothoracic imaging center, Kaohsiung Veterans General Hospital. Kaohsiung Veterans General Hospital-led team developed modified Lung-RADS system for board implementation of lung cancer screening program in Kaohsiung city. The board implementation of LDCT examinations has increased rapidly in recent years, especially after 2011. There has been a 14.63X increase in the volumes of LDCT examinations since 2007 in their hospital. Based on the studies conducted, the gradual implementation of low-dose computed tomography lung screening program could lead to a remarkable decrease in lung cancer mortality (1-year mortality rate 48.16 per centto 37.04 per cent; year mortality rate 88.49 per cent to 69.44 per cent during the period)and a remarkable stage shift in the trend over time(FZ Wu, et al.,2020) shown in Figure 2. Therefore, more people will save their lives because lung cancer diagnosed at early stage.

Conclusion
In summary, prolong implementation of LDCT lung screening program could lead to
lung cancer mortality reduction and stage shiftin the trend over time. The head of the research team suggests that high-risk groups (including those who smoke or do not smoke, age between 40-80 year-old) may consider screening for lung cancer.
To maximize the benefit of LDCT screening and minimize the potential harm in over-diagnosis and over-management among non-smokers, a lung cancer risk prediction algorithm with shared decision-making for pulmonary nodules management is essential for a successful CT lung cancer screening program in Asian population with high prevalence of non-smoking related lung cancer(FZ Wu, et al.,2018).
Conflict of Interest Statement
The authors state they have no conflicts of interest.
References
1. Hsu H-T, Tang E-K, Wu M-T, Wu CC, Liang C-H, Chen C-S, Mar G-Y, Lai R-S, Wang J-C, Wu C-L et al: Modified Lung-RADS Improves Performance of Screening LDCT in a Population with High Prevalence of Non–smoking-related Lung Cancer. Academic Radiology 2018, 25(10):1240-1251.
2. Wu FZ, Huang YL, Wu YJ, Tang EK, Wu MT, Chen CS, Lin YP: Prognostic effect of implementation of the mass low-dose computed tomography lung cancer screening program: a hospital-based cohort study. Eur J Cancer Prev 2020.
3. Wu FZ, Huang YL, Wu CC, Tang EK, Chen CS, Mar GY, Yen Y, Wu MT: Assessment of Selection Criteria for Low-Dose Lung Screening CT Among Asian Ethnic Groups in Taiwan: From Mass Screening to Specific Risk-Based Screening for Non-Smoker Lung Cancer. Clin Lung Cancer 2016, 17(5):e45-e56.
4. Chen PA, Huang EP, Shih LY, Tang EK, Chien CC, Wu MT, Wu FZ: Qualitative CT Criterion for Subsolid Nodule Subclassification: Improving Interobserver Agreement and Pathologic Correlation in the Adenocarcinoma Spectrum. Acad Radiol 2018, 25(11):1439-1445.
5. Wu FZ, Chen PA, Wu CC, Kuo PL, Tsao SP, Chien CC, Tang EK, Wu MT: Semiquantative Visual Assessment of Sub-solid Pulmonary Nodules <==3 cm in Differentiation of Lung Adenocarcinoma Spectrum. Sci Rep 2017, 7(1):15790.
6. Tang EK, Chen CS, Wu CC, Wu MT, Yang TL, Liang HL, Hsu HT, Wu FZ: Natural History of Persistent Pulmonary Subsolid Nodules: Long-Term Observation of Different Interval Growth. Heart Lung Circ 2019, 28(11):1747-1754.
7. Wu FZ, Kuo PL, Huang YL, Tang EK, Chen CS, Wu MT, Lin YP: Differences in lung cancer characteristics and mortality rate between screened and non-screened cohorts. Sci Rep 2019, 9(1):19386.
8. Wu FZ, Kuo PL, Wu CC, Wu MT: The impact of patients' preferences on the decision of low-dose computed tomography lung cancer screening. Transl Lung Cancer Res 2018, 7(Suppl 3):S236-s238.