

More affordable international travel and major advances in medical science, medical or health tourism is becoming less of a novelty and more of a global trend.
In 2007, over half a million Americans travelled abroad to receive medical treatment and since 2003, 1.29 million Britons aged 16 to 64 had dental treatment outside the UK because it was more economical1. These are not isolated trends. Every year, increasing number of patients from around the globe seek healthcare abroad either for economic reasons or to find better quality treatment and overcome long waiting lists. The picture that emerges is of increasing mobile patients with greater choices of where to receive quality treatment at competitive prices.
 Worldwide tourism growth
Worldwide tourism growth
According to the World Travel and Tourism Council (WTTC), tourism is a key driver of 21st century’s economic activity and is the largest creator of jobs, wealth and investment around the world.
It is also the world’s largest export earner with foreign currency receipts from international tourism outstripping exports of petroleum products, motor vehicles, telecommunications equipment, textiles or any other product or service1.
In 2007, international tourist arrivals rose by 6 per cent reaching a new record figure of 898 million and overtaking 2006 figure by over 52 million arrivals. One significant feature of 2007 was the continuing healthy performance of emerging destinations backed up by one of the longest periods of sustained economic expansion2.
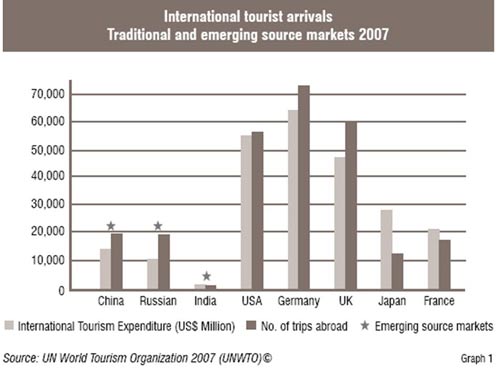
Traditional and emerging source markets 2007
Globally, world tourism flow shows a significant shift from traditional source markets (Western Europe, USA, Canada, Japan) to alternative ones (Central and Eastern Europe, China, Republic of Korea, Singapore, Middle East, Mexico, the Russian Federation, India etc.) Tourism growth has been driven by emerging destinations in Asia, Pacific, Africa and the Middle East, while the more ‘mature’ regions of Europe and the Americas show a more moderate pace.
The increasing trend of health tourism
The increasing trends of tourism coupled with health treatments abroad have led to a growth in the health tourism phenomenon. Health tourism (also called medical tourism, medical travel or global healthcare) is a term initially coined by travel agencies and the mass media to describe the rapidly growing practice of travelling across international borders to obtain healthcare. Such services typically include elective procedures as well as more specialised surgeries such as joint replacement (knee / hip), cardiac, dental and cosmetic surgeries. Travel and leisure aspects typically associated with tourism are now being offered in the form of all-inclusive health tourism packages3.
In 2007, 51 per cent of all international tourist arrivals (430 million) were motivated by leisure, recreation and holidays. Business travel accounted for about 16 per cent (131 million), and 27 per cent represented travel for other purposes such as visiting friends and relatives, religious reasons and / or pilgrimages and health treatment (225 million). Travel for the purpose of undergoing health treatment abroad is clearly on the rise.
Health tourism - An age old concept
The concept of health tourism is not new. The first recorded instance of health tourism goes back to thousands of year when Greek pilgrims travelled from all over the Mediterranean to the small territory in the Saronic Gulf called Epidauria. In the Middle Ages, pilgrims in need of care relied on a network of monasteries providing free, even if basic, care as they made their way slowly to centres such as Santiago de Compostela in what is now called Spain. In eighteenth century England, Mediterranean travellers visited spas as they were places with health-giving mineral waters, treating diseases from gout to liver disorders and bronchitis.
The situation nowadays is very different. First, many people are crossing borders, not on foot or horseback but by trains, cars and increasingly by low-cost airlines. Second, the scope of healthcare has changed beyond recognition with increasingly sophisticated pharmaceuticals and technology allowing many people to survive and in many cases to lead perfectly normal lives6.
Health tourism today - Driven mainly by costs
Highly competitive prices of medical treatment offered abroad continue to attract most medical or health tourists. According to the United Nations World Tourism Organization (UNWTO), depending on the location and procedure, a medical vacation can cost up to 50 per cent, 30 per cent, or even 10 per cent of what one would normally pay at home country2.
The cost of surgery in India, Thailand or South Africa can be a tenth or even less of what it is in the US or Western Europe. For instance, a heart-valve replacement costing US$ 200,000 or more in the US, can go for US$ 10,000 in India including return airfare and a holiday package. Similarly, a metal-free dental bridge worth US$ 5,500 in the US costs US$ 500 in India, whereas the total cost of a standard filling ranges from € 156 in England to € 8 in Hungary. The total cost includes x-rays, materials, drugs and overheads, as well as the dentist’s time. Cosmetic surgery savings are even greater: a full facelift that would cost US$ 20,000 in the US costs about US$ 1,250 in South Africa. A US$ 40,000 hip replacement in the US can cost US$ 6,600 in Costa Rica or US$ 4-5,000 in Cuba. Estimates of the value of medical tourism to India are as high as US$ 2 billion per year by 20124.
The increasing costs of medicare in the US
Consequently, each year more people from the most industrialised nations such as the US are looking for healthcare treatment abroad either for economic reasons or to find better quality treatment and avoid long waiting lists. In a Wall Street Journal-NBC Survey almost 50 per cent of the American public said that the cost of healthcare is their number one economic concern. More and more US citizens are looking beyond their borders for cheaper and more timely healthcare. In 2007 alone, over half a million Americans travelled abroad to receive medical and dental treatment. Part of the reason for US citizens not covered by a universal healthcare system seeking medical care abroad lies in the increasing costs of medicare and private health insurance packages. Nearly 43 million Americans are uninsured and surveys show that the primary reason for this is the high cost of health insurance coverage. Almost 25 per cent of the uninsured reported to change their way of life significantly in order to pay medical bills.
Countries promoting health tourism
Popular medical travel destinations worldwide include: India, Brunei, Cuba, Colombia, Hong Kong, Hungary, Jordan, Lithuania, Malaysia, Philippines, Singapore, South Africa, Thailand and recently, Saudi Arabia, UAE, Tunisia and New Zealand. On the other hand, much sought after cosmetic surgery travel destinations include: Argentina, Bolivia, Brazil, Colombia, Costa Rica, Cuba, Mexico and Turkey. In South America, countries such as Argentina, Bolivia, Brazil and Colombia lead in plastic surgery medical skills relying on their experienced cosmetic surgeons. Colombia also provides advanced care in cardiovascular and transplant surgery. New EU accession countries such as Poland, Hungary and Slovenia offer competitive dental tourism packages particularly to British, German, Austrian and Swiss nationals who can take advantage of budget air travel and cut costs. South Africa is taking the term ‘medical tourism’ literally by promoting their ‘medical safaris’.1
The growth of so-called ‘5-star hospitals’
Most of us are familiar with the star-rating system for hotels, but there is also a growing phenomenon of privately-run ‘5-star’ rated hospitals around the globe in such far-flung places as Bangkok, Singapore, Manila, Kerala and Dubai. These hospitals operate in a highly competitive market and are run along the lines of 5-star hotels. They claim to offer not only medical expertise and state-of-the-art medical technologies, but also first-rate and modern facilities and a wide range of specialised medical and diagnostic services covering all medical disciplines, while guaranteeing more affordable and high quality care for patients.
Increasingly mobile patients
A ‘new’ kind of European and World Citizen is slowly emerging where for instance, a citizen lives and works between two or more countries. This is the case of stockbrokers, bankers and managers who live in financial capital cities during the working week and return home to another country at the weekend or go on holiday to a third country. The term ‘Nylon’ (short for New York-London) has been coined to describe over 400,000 super-commuters who live and work between New York and London (6,500 km, about 5 hours flight), and the term ‘NylonKong” (short for New York-London-Hong Kong) describes commuters, often financial service executives, who commute regularly between London, New York and Hong Kong. There are no less than 187 direct flights that leave London for New York every week and 28 weekly flights from Hong Kong to New York. This category of upwardly mobile professionals on the move is a major target for health tourism.
The increasing mobility of pensioners in Europe is also an emerging trend. Northern European retirees are taking up residence in South European countries and the Mediterranean for part of the year during the coldest winter months of the year. They are estimated to be over 800,000 annually in the European Union (EU). In the Lake Garda area of the Veneto Region in Northeast Italy, there are over 3,500 permanent residents from Northern Europe. According to the UK Office of National Statistics, one million Britons have decided to move overseas after retirement, with Spain being their popular choice. In the last 10 years, over 75,000 British pensioners have moved to Spain to establish permanent residence6.
 Challenges to patient mobility and health tourism
Challenges to patient mobility and health tourism
The increasing mobility of citizens in the EU and the growth of global health tourism present a number of challenges. Firstly, standards are important as far as healthcare is concerned and issues concerning international health accreditation, evidence-based medicine and quality assurance need to be addressed. In the US, Joint Commission and in the UK and Hong Kong, the Trent International Accreditation schemes provide certain guarantees of standards and quality of healthcare of affiliated hospitals and healthcare institutions. However, there is still a long way to go before such accrediting bodies can cover the vast range of healthcare providers worldwide.
With the progressive introduction of the European Health Insurance Card in Europe on 1st June, 2004, EU citizens could obtain essential medical treatment while staying abroad temporarily or exercise their right to better quality and more timely planned care in another Member State if waiting lists force them to seek alternative treatment abroad. Treatment is provided in accordance with the rules of the Member State being visited and costs are reimbursed in line with the tariffs applied in that Member State.
The right to safety and quality care is an essential element for all patients in Europe. Each individual has the right to choose among different treatment procedures and providers in various Member States and to receive treatment without any delay. This is true within national healthcare systems in accordance with article 22.2 of EC Regulation 1408/71 and to further rulings of the Court of Justice. The question is whether it always works in practice.
Accessing healthcare in another European country should theoretically be a straightforward process, but it often creates problems both for patients and the healthcare systems involved. The experience of certain European areas with heavy tourist flows (as is the case of the Veneto Region in Italy outlined below) is a clear example of the extent of the tourism phenomenon, which implies actions at different levels (regional, national and European), further implying particular legal, organisational and regulatory approaches6.
The impact of tourism on the Veneto Region, Italy: A case study
The Veneto Region in its capacity as a highly popular tourist destination, makes a very interesting case study of patient mobility and health tourism in Europe. The significant flow of tourists brings with it a series of healthcare challenges that regional healthcare services have to deal with, in some cases by organising specific services to respond to the high demand of seasonal tourist flows and long-term foreign residents and ensuring their good health.
During the last decade, the Veneto Region of northeast Italy has become famous as a major tourist destination, thanks to three main attractions: Venice, as a city of art and culture along with Verona, Padua and Vicenza, the Mediterranean beaches of the Adriatic sea; the lake region (Lake Garda); and the Dolomite mountains2. Economically, tourism has become one of the Veneto’s main resources. In 2006, spending1 by foreign visitors to the Veneto totalled € 3,845 million—15.9 per cent of total spending by foreign visitors in Italy.
Nowadays, visitors to the Region can in case of a medical emergency choose from a wide range of health services provided by its Local Health Authorities (LHAs) in close collaboration with the Department of Health and Social Services and the Department of Tourism of the Veneto Region.
The Veneto Region ranks number one among the Italian regions in terms of tourist flows (see Table 1).
National and international tourist flows to the Veneto Region, year 2006

Source: Veneto Regional Statistics Office data based on ISTAT 2006
Looking at the tourist flows to the Veneto Region in 2006, we can clearly see the following: Foreign tourist arrivals mainly from Germany (1,888,235), Austria (642,886), the UK (592,926), France (521,043), Spain (387,330) Non-EU countries, mainly the USA (818,262), Japan (280,601) and Australia (118,053) make up the greater proportion of total overnight stays amounting to over 59 million.
Health tourism to the Veneto Region
The Veneto Region’s health services are facing challenges mainly from mass tourism, which brings with it a sudden and significant increase of demand on health services, particularly in the summer with different priorities depending on the type of tourism, for example cultural, seaside, agro or adventure tourism.
 Since 2003, a special ‘task force’ has been formed in the Veneto with the aim of broadening the knowledge of the tourism phenomenon and patient mobility, and to cope with the underlying administrative and organisational problems. Its aim is to collect and provide data on the magnitude of the phenomenon of patient mobility between the Veneto Region and other regions or Member States and to analyse the impact of cross-border health demand and related health issues at the regional level6.
Since 2003, a special ‘task force’ has been formed in the Veneto with the aim of broadening the knowledge of the tourism phenomenon and patient mobility, and to cope with the underlying administrative and organisational problems. Its aim is to collect and provide data on the magnitude of the phenomenon of patient mobility between the Veneto Region and other regions or Member States and to analyse the impact of cross-border health demand and related health issues at the regional level6.
 Conclusion
Conclusion
Trends clearly point to a continued expansion of medical tourism in the coming years. However, there is an urgent need to provide and compare private and NHS health services for tourists, and to be aware of the risks involved and the legal implications resulting from medical complications that may arise on the patient’s return to home.
Furthermore, international standards of quality assurance and health accreditation need to be established to protect citizens worldwide and ensure them their rights to the best healthcare possible at the most competitive prices.
We are now at the dawn of a new era in health tourism worldwide, where citizens have more options as regards where they choose to be treated and how to spend their money.
By 2015, the health of the so-called Baby Boomer generation will have started to decline. With more than 220 million Baby Boomers in the US, Canada, Europe, Australia and New Zealand, this represents a significant market for cost-effective and high-quality medical care, and has enormous potential for global health tourism.
AUTHOR BIO
Luigi Bertinato is the Director of International Health and Social Affairs Office, Department of Health and Social Services, Veneto Region, Venice-Italy. He is involved in a number of European health and social care projects, in the area of health policy, e-health, health promotion and patient mobility.
Marina Canapero is the Health Communications Consultant, International Health & Social Affairs Office, Veneto Region. Since 2003, she has been collaborating part-time as a consultant in the International Health & Social Affairs Office of the Veneto Region in Venice, liaising with
References
1. UNWTO Tourism Highlights 2007 Edition, UNWTO Publications.
2. UNWTO World Tourism Barometer, Vol. 6, N.1, January 2008
3. Hutchinson B. Medical Tourism Growing Worldwide. University Of Delaware. Available on http://www.udel.edu/PR/UDaily/2005/mar/tourism072505.html.
4. Bertinato L, Busse R, Fahy N et al, Policy Brief on Cross-border Health Care in Europe, European Observatory on Health Systems and Policies
5. Scaramagli A, Zanon D, Ronfini F, Bertinato L, Toniolo F, Chapter 6, Health care for tourists in the Veneto Region in Patient Mobility in the European Union, Learning from Experience, Rosenmöller M, McKee M, Baeten R, World Health Organization 2006, on behalf of the Europe 4 Patients project and the European Observatory on Health Systems and Policies.
6. The Veneto: sharing facts - comparing facts, Statistical Report 2007. Available at: http://statistica.regione.veneto.it/ENG/pubblicazioni_elenco.jsp
7. McKee, M., and Nolte E. (2004). The Implications for Health of European Union Enlargement. British Medical Journal,;328:1025-1026.






