

The heart, inadequate blood supply, and revascularisation
The coronary arteries supply the heart itself with oxygen and nutrients. Severe narrowing of these coronaries (stenosis) might lead to chest pain or a heart attack. Myocardial revascularisation by either percutaneous coronary intervention or coronary artery bypass graft (CABG) improves symptoms, quality of life and survival in these patients. A stenosis with a diameter reduction < 50 per cent is considered a mild stenosis, 50 – 70 per cent as moderate, and > 70 per cent as severe. Unfortunately, the degree of coronary stenosis can easily be overestimated and impacts short and long-term outcomes of CABG.
A heart lung machine takes over the heart’s pumping function and gas transfer of the lungs during heart surgery. Major drawbacks, however, are a systemic inflammatory response, acute kidney injury or brain infarctions. For CABG, the heart lung machine can be abandoned by performing off-pump coronary artery bypass grafting where the heart keeps beating during surgery.
Intraoperative choices and challenges lead to postoperative complications
Patients’ own arteries from the chest or lower arm can be used to create these coronary bypasses. These arterial grafts have excellent long-term functionality, and low redo revascularisation rates. Arterial grafts require proper handling to avoid early technical failure. Competitive flow from native coronaries that are not narrowed enough impacts long term success of the coronary bypass. Detection of competitive flow for arterial grafts as early as possible after making the anastomosis might predict the longterm patency.
Intraoperative assessment of graft flow can be measured with transit time flow measurements (TTFM). European guidelines on myocardial revascularisation suggest routine use of intraoperative bypass graft flow assessment. Unfortunately, this quality control technique is not always used, nor handled upon adequately during surgery. The first signs of a failed graft are heart rhythm changes, postoperative new onset of chest pain and a potential myocardial infarction might occur. Often, the patient already left the operating theatre, and bypass graft revision is not possible, or should be considered for another surgical procedure.
Cut-off values for TTFM to indicate graft failure are still debated, and are not uniform between clinical studies. In a recent study conducted at Thoraxcentrum Twente of Medisch Spectrum Twente (Netherlands), preoperative angiography findings were combined with intraoperative TTFM in 50 CABG patients without the use of a heart lung machine (off-pump CABG). All patients had significant coronary artery disease as established by heart team discussion between a cardiologist and heart surgeon.
Temporary closing of a severely narrowed coronary artery
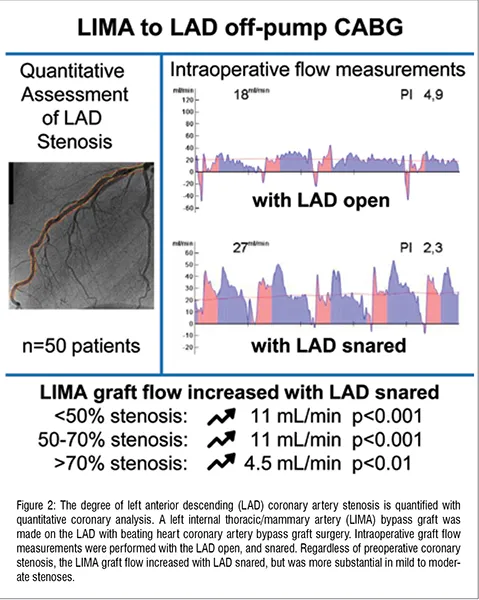
During off-pump CABG, a bypass graft was made with the left internal thoracic artery (LIMA) on the largest coronary artery on the front side of the heart (left anterior descending artery, LAD). This coronary artery was then temporarily closed and the bypass graft flow was measured with TTFM. Hereafter, a new measurement was performed with the coronary artery reopened. After the initial bypass graft, arterial grafts were placed to other parts of the heart.
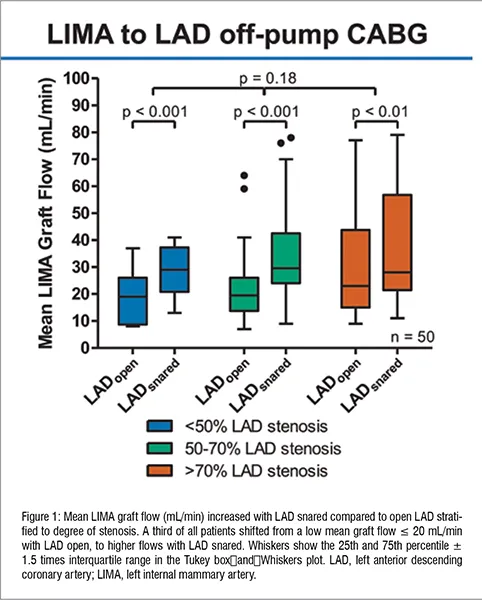
As expected, higher values of bypass graft flow were observed with the coronary artery snared, effectively preventing any competitive flow. More interestingly, the mean graft flow increased from 20 mL/min with open LAD to 30 mL/min with snared LAD and differed between severity of coronary stenosis groups (Figure 1). In more than half of the patients (52 per cent) the mean graft flow was lower than clinical relevant TTFM cut-off values with the LAD open. Graft flow increased in 16 patients after snaring the LAD, and shifted to acceptable TTFM values. This increase might indicate an open, and functional anastomosis affected by competitive flow from the native coronary artery. Here, surgical graft revision will not likely improve baseline TTFM values such as mean graft flow or graft patency, resulting in a useless or even harmful procedure.
Is snaring safe?
Snaring the LAD is a widespread method to obtain a bloodless operative field, and is well tolerated by patients. Indeed, this technique is comparable to intracoronary shunting regarding postoperative heart enzyme rise. Atherosclerotic plaques or calcified coronary arteries make shunting technically more tough. Prolonged snaring might induce blood vessel injury, and arrhythmias, but are reversible up to 20-30 minutes of snaring.
Patient-specific decision making before and during surgery
Patient-specific decision making is performed daily in heart team discussion between cardiac surgeons and cardiologists according to international guidelines. Here patient characteristics determine decision making for a surgical, percutaneous or conservative treatment. Combining patient characteristics with procedural characteristics could further tailor treatment and thus improve outcomes for patients.
Professional information for decision making is scattered. Direct comparison between competing treatments or diagnosis modalities is often lacking. For assessing coronary artery stenosis, visual eyeballing by a cardiologist is most common, although high intra-and inter-observer variability exists for many years with low concordance around clinical relevant cut-off points. Some centres use quantitative coronary analysis (QCA) with 2D or 3D reconstruction using cardiac angiography to analyse degree of stenosis for research purposes, but are rarely used for heart team discussions. To predict graft patency, it is no match compared to functional assessment using the more invasive fractional flow reserve (FFR). Here, clinical cut-off values are also debated and might even differ between percutaneous coronary intervention or CABG. Future studies should investigate the cut-off values of FFR or QCA for PCI and CABG to optimise outcome for patients.
Implications for daily practice
Heart time discussions should carefully, and objectively evaluate the functional degree of coronary stenosis to determine revascularisation strategies. Because preoperative visual estimation proves to be difficult, intraoperative evaluation of a stenosis is pivotal. Routine snaring of the LAD during off-pump CABG demonstrated an increase in mean graft flow among all coronary stenosis groups. A third of clinical cut-off TTFM values for graft failure shifted to acceptable values. Therefore, regular use of TTFM and careful analysis of competitive flow according to the method described in the underlying study can be useful to identify competitive flow in case of intraoperative borderline TTFM parameters. Adequate intraoperative quality control improves patients postoperative quality of life, reduces lifeevents such as myocardial infarctions or unnecessary graft revisions, and therefore reduces hospital costs of prolonged treatments.
Clinical studies should establish definitive evidence regarding routine snaring of the LAD during off-pump CABG. These studies should focus on the prevention of unnecessary intraoperative graft revisions and postoperative heart attacks.


