Precision Medicine in Allergy-Asthma

Allergy-asthma is an enormous burden on healthcare systems and its health impact is substantial. This article describes scientific information on what allergy is, how allergy responses occur, what are the symptoms, how to diagnose it and a word about medications.
According to the World Health Organisation (WHO), more than 20 per cent of the world population suffers from IgE (Immunoglobulin E) mediated allergic diseases such as allergic asthma, allergic rhino-sinusitis, allergic conjunctivitis, eczema/atopic dermatitis and anaphylaxis. The recent Global Burden of Disease (GBD, 1990-2019) estimated total burden of asthma in India at 34.3 million, accounting for 13.09 per cent of the global burden. The health impact of allergy-asthma is substantial and the burden is increasing owing to climate change and adverse environmental factors.
Asthma is a Greek word meaning “panting”. The Global Initiative for Asthma (GINA) defines it as a heterogeneous disease usually characterised by chronic airway inflammation. Elaborating it, the presenting symptoms as well as treatment responses differ person-to-person and hence it is important not to adopt “one size fits all” or blanket solutions for all asthmatics. These patients require proper understanding of their household as well as work environments and personalised care plans to achieve maximum symptom control. In short, the need of the hour is to practice precision medicine to answer most common questions encountered in clinical scenario:
1. What am I allergic to?
2. Can my allergy be cured?
The following description will help understanding allergy-asthma scientifically. It will also provide information on latest technologies to find out precise culprits and shed lights on hope for allergy cure.
What is allergy?
The term “Allergy” was coined by von Pirquet in the year 1906. With it he wanted to describe a change in reactivity. In general, allergy occurs when a person reacts to substances known as allergens, which are harmless, non-infectious and in abundance in the surrounding environment. A person’s inherent tendency of being hypersensitive to particular substance is known as atopy. According to Gell and Coomb, the hypersensitivity reactions are classified into four types based on involvement of different cells and mediators.
Allergic reactions are most commonly attributed to Immunoglobulin E (IgE) mediated or Type 1 hypersensitivity reaction. IgE is part of the human body’s immune system. Its level rises in serum on allergen exposure which ultimately is responsible for symptoms of allergy.
SYMPTOMS OF ALLERGY
When a predisposed or atopic individual is exposed to an allergen, the body reacts in a way to eliminate the offending substance out of the body with different behavioural responses like itching, rashes, running nose, sneezing, coughing and watering of eyes. However, in some persons it can lead to inflammation/ swelling and narrowing of airways which causes wheezing and difficulty in breathing — the main attributes of asthma. In some cases it can lead to life threatening anaphylaxis, where the body goes into complete shock.
These symptoms can be seasonal or perennial (year round). Most often it is found that symptoms increase due to triggers. Exposure to smoke, heavy perfumes or pungent smell, air pollution, difference in temperature or humidity as well as emotional stress can trigger allergy-asthma symptoms. As allergic tendencies run in families, positive family history contributes significantly in diagnosis of allergy.
Allergic March
Though allergies most commonly manifest as rhinitis/dermatitis, according to a school of thought, it can progress to asthma or life threatening allergies if not addressed in time. The phenomenon is called “allergic march”. It is observed many times that a person first has upper respiratory tract allergies and limited symptoms but it slowly progresses to chest congestion and wheezing with increase in severity and frequency over time. There are no tests yet which can predict development of allergy-asthma or its progression. In that scenario, the best way is to keep regular follow up check up.
Diagnosis
Traditionally, skin prick testing (SPT) was considered as gold standard of allergy diagnosis. In this, a drop of crude allergen extract is placed over the forearm/back and it is pricked with a lancet. The positive response is noted by development of wheel and flare. This roughly hundred years old technique suffers the drawback of purity of allergen extracts as well as issues of cross-reactivity. Due to poor cooperation this technique is not suitable for diagnosis in children.
The other alternative is called in-vitro tests where the blood is tested for presence of IgE against particular allergen. IgE assays based on ELISA/ EIA are sensitive but not specific. The capture assays are slightly more specific. However, these in-vitro tests S. IgE against carbohydrate, lipid and protein: all three components of allergen. As only the protein component is responsible to mediate allergenic responses, IgE measured against other two may lead to false positive reports. The issue of crossreactivity still persists and for the same reason, these tests detect ‘sensitivity’ and not true allergy. Hence there is a dire need of precision diagnostic testing to identify the culprit allergens.
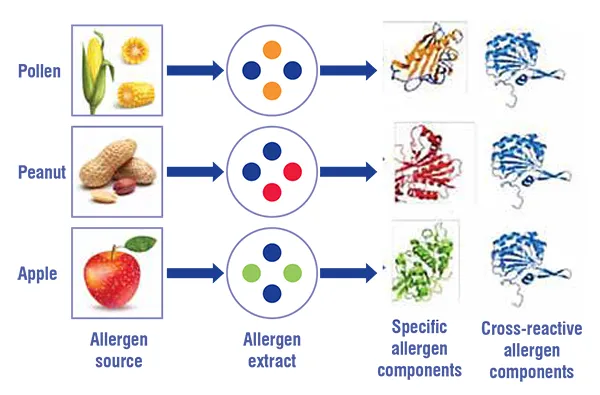
Precision diagnosis with CRD allergy profile
Component resolved diagnosis (CRD) allergy profile is an in-vitro method, where the patients’ serum is tested for specific IgE levels against approximately 300 known allergens. In this method, IgE level against only protein moieties of purified and filtered allergenic extract, the specific components responsible for allergic responses, is measured. In addiction, cross-reactive carbohydrate determinant (CCD) inhibitors makes it possible to cancel noise. Presence of IgE in substantial levels against major allergen components is considered a hallmark of allergy diagnosis. The test is reasonably sensitive and specific. However Indian studies are still awaited as the test is available only in few entres
across India.
For example, a person suffering from apple allergy, the reactions can be prevented if the apple is given after peel removal as suggested by CRD allergy profile. Cockroach allergies can be controlled with robust pest control measures. Pollen and Mould allergies can be controlled with appropriate environmental intervention. Most importantly, dust mite sensitisation can potentially be cured.
Allergy cure: Is it possible?
Allergen immunotherapy (AIT), a scientific method where the offending allergen is administered, mostly via subcutaneous route, to develop immune tolerance, has potential to allow a symptom- and medication-free life. Known as allergy shots, these can lead to long-term benefits provided the treatment is based on sound knowledge of presence of IgE against major allergen zomponent, mainly dust mites, and administered after thorough evaluation like spirometry and detailed physical examination at an experienced centre and for appropriate duration.
After careful selection, in a person suffering from dust mite allergy, AIT administered in build up and maintenance phase can slowly lead to reduction of allergen-specific IgE levels and convert it to an IgG mediated response, which will no longer produce the symptoms. Though it may sounds simple, it is best carried out only under professional guidance and at an experienced centre.
Medications
The goal of an allergy-asthma treatment plan is to reduce the risk and symptoms. The subset of patients deemed unfit for successful administration of AIT have medications and allergen avoidance as mainstay of treatment plan. The medications can be divided according to their role: preventer/controller medications and reliever medications. Reliever medications are used after the symptoms have appeared and mainly tame the aggravated symptoms. While preventer/controller medications need to be taken on regular basis, irrespective of symptoms, to be adjusted after re-assessment at scheduled interval, which is usually around 6-12 weeks. Rapid withdrawal of preventer/controller medications or poor adherence to same are major risk factors for frequent flareups as well as asthma with fixed airway obstruction.
References:
1. https://apps.who.int/iris/bitstream/handle/10665/68361/WHO_NMH_MNC_CRA_3.2.pdf
2. https://openres.ersjournals.com/content/8/2/00528-2021. ERJ Open Research Apr2022, 8 (2) 00528-2021; DOI: 10.1183/23120541.00528-2021
3. https://www.worldallergy.org/education-and-programs/education/allergic-disease-resource-center/professionals/allergic-asthma-symptoms-and-treatment
4. https://ginasthma.org/gina-reports/
5. Huber B. 100 Jahre Allergie: Clemens von Pirquet - sein Allergiebegriff und das ihm zugrunde liegende Krankheitsverständnis [100 years of allergy: Clemens von Pirquet - his idea of allergy and its immanent concept of disease]. Wien Klin Wochenschr. 2006 Oct;118(19-20):573-9. German. doi: 10.1007/s00508-006-0701-3.PMID: 17136331.
6. https://www.aaaai.org/Tools-for-the-Public/Allergy,-Asthma-Immunology-Glossary/Atopy-Defined
7. Rajan TV. The Gell-Coombs classification of hypersensitivity reactions: a re-interpretation. Trends Immunol. 2003 Jul;24(7):376-9. doi: 10.1016/s1471-4906(03)00142-x. PMID: 12860528.
8. Abbas M, Moussa M, Akel H. Type I Hypersensitivity Reaction. 2021 Jul 21. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. PMID:32809396.
9. https://gpnotebook.com/simplepage.cfm?ID=x20120321132301331321
10. Bantz SK, Zhu Z, Zheng T. The Atopic March: Progression from Atopic Dermatitis to Allergic Rhinitis and Asthma. J Clin Cell Immunol. 2014 Apr;5(2):202. doi: 10.4172/2155-9899.1000202. PMID: 25419479; PMCID: PMC4240310.
11. https://www.aafa.org/allergy-diagnosis/
12. Heiss S, Mahler V, Steiner R, Spitzauer S, Schweiger C, Kraft D, Valenta R. Component-resolved diagnosis (CRD) of type I allergy with recombinant grass and tree pollen allergens by skin testing. J Invest Dermatol. 1999 Nov;113(5):8307. doi:10.1046/j.1523-1747.1999.00796.x. PMID: 10571741.
13. https://www.allergy.org.au/patients/allergy-treatment/immunotherapy#:~:text=Allergen%20immunotherapy%20is%20the%20closest,over%20a%20period%20of%20years.
14. InformedHealth.org [Internet]. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG); 2006-. Medication for people with asthma. 2008 Jan 14 [Updated 2017 Nov 30]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279519/

