Trans-carotid TAVI
The French alternative

This article is related to the carotid approach for TAVI, and shows comparable outcomes in terms of 30 days mortality, strokes and vascular complications in 500 consecutive patients. Trans-carotid TAVI has become our first alternative in case of femoral contraindications.
Introduction
TAVI is now a daily practice for the treatment of aortic stenosis. The question today is to choose the best approach for each patient.
All the competences of the heart team must be used to obtain the best results.
The common carotid artery: straight on to the aortic ring
Anatomical characteristics, like iliofemoral stenosis or abdominal aortic aneurysms, required to find another way to reach the heart safely for TAVI. Despite their good results, the classical alternatives such as the apical or aortic routes are not comparable to the femoral one in terms of surgical approach and operative burden. The subclavian artery is a fragile artery and with a delicate surgical control.
The common carotid artery (right or left), which is very simple to control, is a large artery offering a privileged access to the aortic ring.
Approached on its first centimeters, the proximity of the puncture point and the valve allows an excellent adjustment of the height of the prosthesis during the delivery.
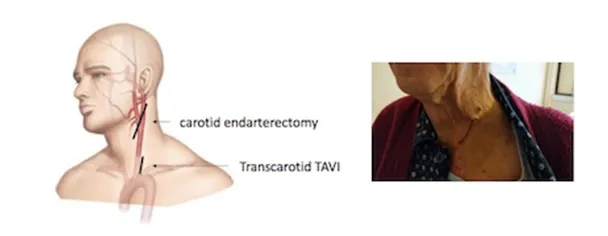
Figure 1: Incision for surgical approach of the left common carotid artery.
A minimally invasive procedure!
Trans-carotid TAVI can be performed under local or general anesthesia.
Intervention is perfectly comparable to the femoral approach.
The optimised procedure, with radial puncture and stimulation on the left ventricle stiff wire, allows an early rehabilitation, without any danger of bleeding on the femoral artery.
A small drain (8Fr) is placed in the incision and removed on day one. Then, the patient benefits from the same post-operative monitoring protocol as femoral patients.
Simple as a femoral intervention
In a hybrid room or in the operating theatre with a mobile C-arm, the endovascular material is the same as the femoral route.
Pigtail angiography catheter is introduced in the aortic root through the radial or femoral artery under ultrasound guidance. Rapid pacing is done with a right ventricle probe introduced throughthe femoral or left jugular vein.
A straight guide wire, usually directed by an AL probe, is used to cross the aortic valve, and the SAFARI (Boston Scientific) is set up.
The Commander femoral introducer (Edwards) limits arterial trauma and balloon-prosthesis alignment is easily achieved in the ascending aorta.
The Certitude introducer (Edwards), dedicated to classic alternative surgical routes, or the Medtronic Corevalve system is also perfectly adapted.
Concretely
Installation for a carotid procedure with the Commander delivery system requires some space at the top of the patientbut does not present any particular difficulties.
The operating table is moved as far as possible towards the feet and an instrument table is placed on top.
If the OR is too small, the Certitude surgical introducer can be used.

Figure 2 : Installation
Once the common carotid artery is controlled, the sheath is introduced following a classic Seldinger puncture under visual control.
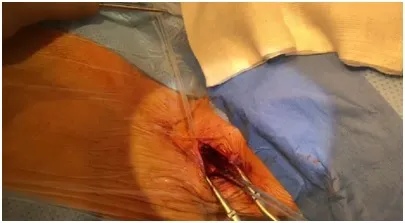
Figure 3: Control of the common carotid artery
The introducer is then placed under fluoroscopic control in the aortic arch just above the ostium of the common carotid artery.
The device can be fixed with a stitch on the skin
The reactivity of the material is facilitated by the proximity of the puncture point and the straightness of the device. High placement of the prosthesis in the aortic annulus is thus easier, in the hope of limiting conductance disorders.
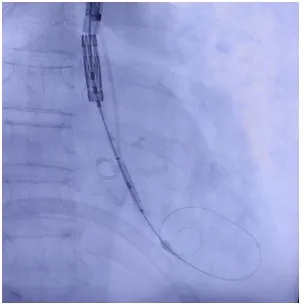
Figure 3: Balloon Alignment in the ascending aorta
At the end of the procedure, the common carotid artery is surgically repaired with separate stitches of 6-0 Prolene, allowing non-stenotic restoration of the lumen.
Identical pre-operative assessment
Internal carotidstenosis was systemically assessed by supra-aortic Doppler ultrasound and in a few cases with a dedicated CT.
In patients with significant stenosis (>70 per cent) at the carotid bifurcation, the most affected side was chosen for the intervention. TC-TAVR was excluded in case of bilateral significant carotid stenosis (>70 per cent).
The absence of calcifications in the first centimeters of the common carotid artery is easily visualised on the TAVI scan. The tortuous nature of the arteries, except in extreme cases, does not represent a limitation since the carotid artery is easily mobilised and the stiff guide wires makes it straight.
Comparable results and no more strokes
Our article(1), recently published in the European Journal of Cardio-Thoracic Surgery, compares 100 consecutive carotid patients with 400 patients treated through the femoral route in Nantes.
This work shows comparable results, including 98 per cent procedural success in both groups, similar in-hospital mortality (2 per cent vs. 1 per cent, p=0.345) and stroke rates (2 per cent vs. 2.5 per cent, p>0.999).
The surgical approach resulted in a very low rate of major vascular complications (2 per cent vs. 4 per cent, p=0.548) and greatly limited minor complications such as hematomas at the puncture site (6 per cent vs. 12.8 per cent, p=0.077).
Our results corroborate other carotid series (2–5)and do not show a risk of stroke attributable to the carotid route, too often considered as a limitation.
Perspectives
The simplicity and encouraging results of carotid TAVI have gradually led us to use this approach routinely in patients not eligible for the femoral route.
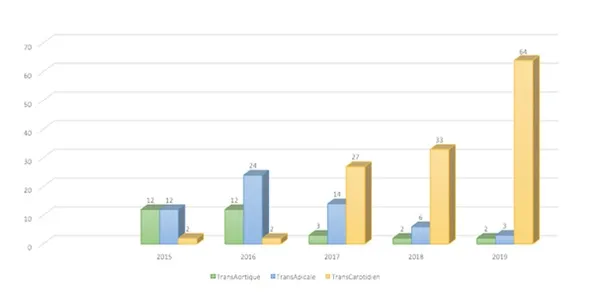
Figure 4: Evolution of non-femoral approaches at Nantes University Hospital since 2015
The safety of the carotid route now demonstrated, it no longer seems reasonable to push the indications of femoral TAVI on poor quality vessels or on hard-to-reach vesselsas in obese patients.
The cohesion of the Heart-Team seems once again to be the only solution to propose the best for our patients.
References:
1. Marie B, David CH, Guimbretière G, Foucher Y, Buschiazzo A, Letocart V, et al. Carotid versus femoral access for transcatheter aortic valve replacement: comparable results in the current era. Eur J Cardiothorac Surg. 16 mars 2021;ezab109.
2. Mylotte D, Sudre A, Teiger E, Obadia JF, Lee M, Spence M, et al. Transcarotid Transcatheter Aortic Valve Replacement: Feasibility and Safety. JACC Cardiovasc Interv. 14 mars 2016;9(5):472‑80.
3. Watanabe M, Takahashi S, Yamaoka H, Sueda T, Piperata A, Zirphile X, et al. Comparison of Transcarotid vs. Transfemoral Transcatheter Aortic Valve Implantation. Circ J Off J Jpn Circ Soc. 25 2018;82(10):2518‑22.
4. Wee IJY, Stonier T, Harrison M, Choong AMTL. Transcarotid transcatheter aortic valve implantation: A systematic review. J Cardiol. 2018;71(6):525‑33.
5. Folliguet T, Laurent N, Bertram M, Zannis K, Elfarra M, Vanhuyse F, et al. Transcarotid transcatheter aortic valve implantation: multicentre experience in France. Eur J Cardio-Thorac Surg Off J Eur Assoc Cardio-Thorac Surg. 1 janv 2018;53(1):157‑61.








